- The Arrow
- Posts
- The Arrow #248
The Arrow #248
Michael Eades
October 03, 2025
Hello friends.
I didn’t know how the Big River piece was going to fly last week. I was surprised to see such a positive response. MD and I took the kids to NY to see Big River on Broadway in 1985. It was their first time to see a Broadway show, and the whole thing was magical…except for the part where our youngest came within a hair’s breadth of being run over on the way to the theater. He came even closer several years later when we were visiting Charles Dickens’s house in London. He tried to dart across a street where traffic was going the wrong way—for Americans, at least. He really almost bought it there.
Roger Miller wrote the music and lyrics to Big River, which won 7 Tony Awards, including Best Score for Miller.
Roger Miller started out composing songs for other singers. He was kind of a mad genius musically. He taught himself to play a number of instruments, and could whip out a song in no time. It took him all of four minutes to write Dang Me, which is one of my favorites. Along with writing all kinds of so-called novelty songs, he sprinkled a few serious ones in there along the way.
His first big hit as a singer was King of the Road, which I wasn’t all that crazy about. But it really put him on the map. It was a mega best seller, and after it came out, Roger Miller was everywhere in the late 1960s. He even had his own TV show.
When I was working the worst job I’ve ever had in my life as a conductor on the train that runs around Disneyland, Roger, his wife, and two kids got on my train car. This was right after King of the Road had come out, and no one recognized him. But I did as I was a huge fan. I said, “Hi, Roger.” He replied in his Oklahoma twang, “Can you believe this is the first time I’ve ever been on a train.” For those who aren’t Miller fans, King of the Road is all about hobos and trains.
He wrote so many weird songs, one wonders how he could even come up with the idea. Here’s another of my favs from back in the day. I mean who would ever think of writing a lyric about the wind from a big semi truck going by and whipping the big legs of one’s Levis. Only Roger.. But as they say IYKYK.
One of the songs Roger composed for others was In the Summertime, which Andy Williams made into a huge hit. Here is a video of the two of them singing it in their different styles. Don’t feel bad for Roger’s hang dog look about how his version died on the vine. He probably made more money on it than Andy Williams did. Roger got writing credit each time it played on the radio—Andy didn’t get squat. Andy got paid only for performances and records sold. Roger got paid every time the song was played anywhere, no matter who sang it.
Okay, enough about Roger Miller. I’m going to give you one last dose of him on the VOTW. It was a surprise to our family when we went to see the Broadway version.
The Arrow is a reader-supported guide to nutrition, medicine, books, critical thinking & culture. Both free and paid subscriptions are available. If you would like to support my work, the best way is by taking out a paid subscription.
Okay, from Roger Miller and fun to the treachery of Pfizer
Despite It’s Long Criminal Past, Pfizer Weasels It’s Way Into Trump’s Good Graces
President Trump just can’t seem to break free from the death grip Pfizer and it’s president Albert Bourla has on him. Given their sorry performance with the Covid vaccines, I was hoping Bourla and Pfizer would be exiled from the White House. But I guess the world’s largest pharmaceutical company is a force with resources large enough to weather all that. And that’s not to mention all those in the house and senate on Pfizer’s payroll, who have the president’s ear.
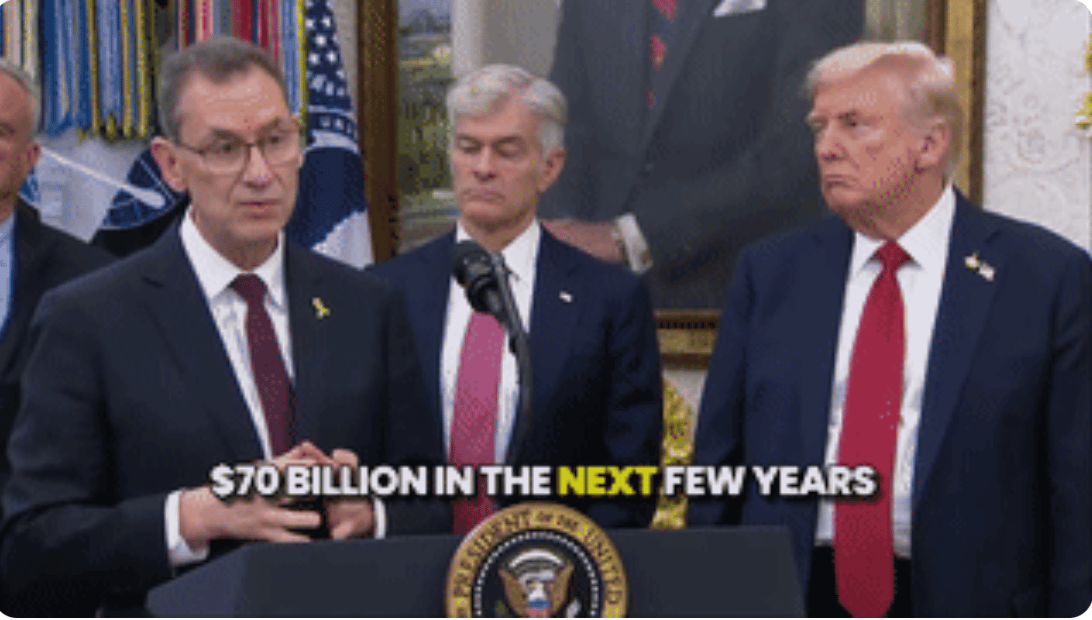
Here is almost the perfect photo. Bourla is on the left. Dr. Oz is in the middle. At first glance, I thought Dr. Oz was Senator Bill Cassidy, who would be standing there with his hands in Bourla’s pocket. Cassidy is RFK’s nemesis in terms of getting done what he wants to get done. Cassidy takes big bucks from Big Pharma and he doesn’t want to risk that, so he fights RFK every step of the way. Then there is President Trump, who believes the discount Pfizer is going to provide for Medicaid only will end up saving “millions of dollars.”
Total health care spending in the US is at about the $4.9T (T, not B) per year, so a few hundred millions of dollars isn’t even a rounding error. And for this, Trump is letting this fox back in the henhouse.
In case you’ve thought Pfizer is another drug company like all the rest, just a little larger, you need to be aware of it’s criminal actions over the past couple of decades.
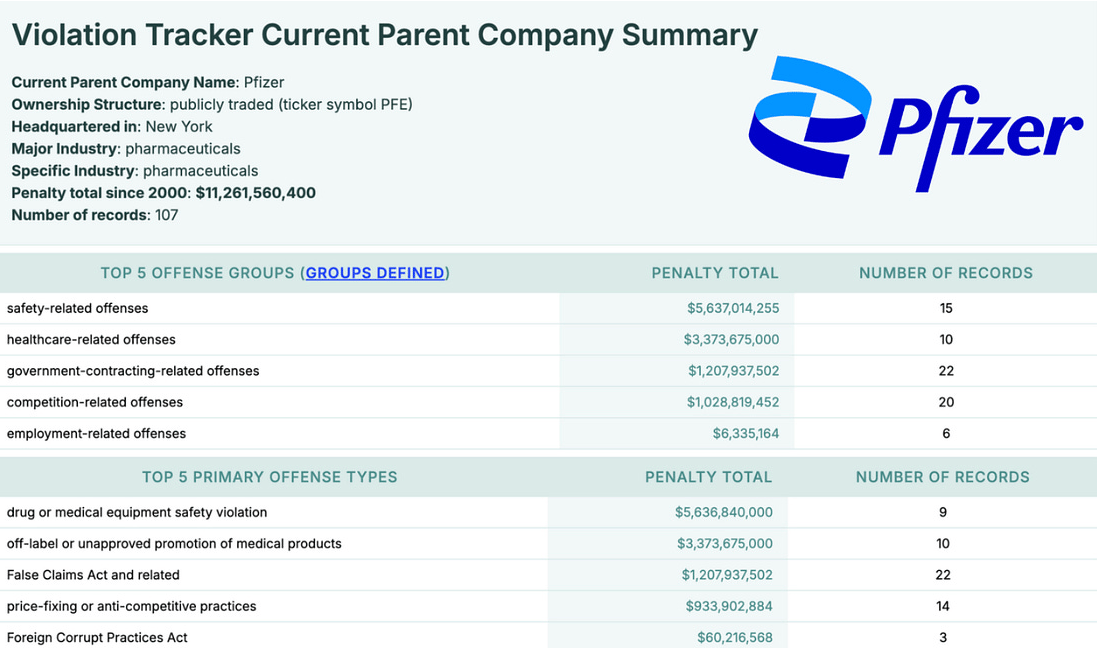
And Pfizer isn’t just a drug company; it is a criminal entity as well. According to researcher Nicolas Hulscher, Pfizer has a long history of criminal charges and huge criminal fines.
Pfizer’s rap sheet includes some of the largest criminal fines in U.S. history:
In 2009, Pfizer and its subsidiary Pharmacia & Upjohn reached a record $2.3 billion settlement with the U.S. Department of Justice. Pharmacia & Upjohn pleaded guilty to a felony charge of misbranding Bextra and paid a $1.195 billion criminal fine. At the same time, Pfizer Inc. agreed to pay $1 billion under the False Claims Act to settle allegations of illegal promotion, false billing to Medicare/Medicaid, and kickbacks to prescribers. In 2004, Warner-Lambert (acquired by Pfizer in 2000) pleaded guilty to two felony counts for illegally promoting Neurontin, paying $430 million in combined criminal fines and civil liabilities. Over the years, Pfizer has paid out billions more for unlawful marketing practices, Medicare/Medicaid fraud, and physician kickbacks.
According to Violation Tracker, Pfizer’s penalties since 2000 total more than $11 billion across criminal, civil, and regulatory cases — a staggering figure that exposes a pattern of lawlessness, not isolated mistakes.
Despite all this out-and-out criminality, the White House is handing out a reward of $90B to Pfizer to put towards its mRNA empire. One of the things being talked about is using the mRNA platform for allergy shots. (!!!) Even given the many reports of the mRNA products spreading from the injection site to many parts in the body. Same with the lipid nanoparticles. Covid, in the minds of many, was a serious illness, especially in the elderly and those with multiple co-morbidities, so it was a different risk-reward calculation than there would be as a treatment for allergies. I certainly wouldn’t be willing to take the risk.
Tylenol and Autism
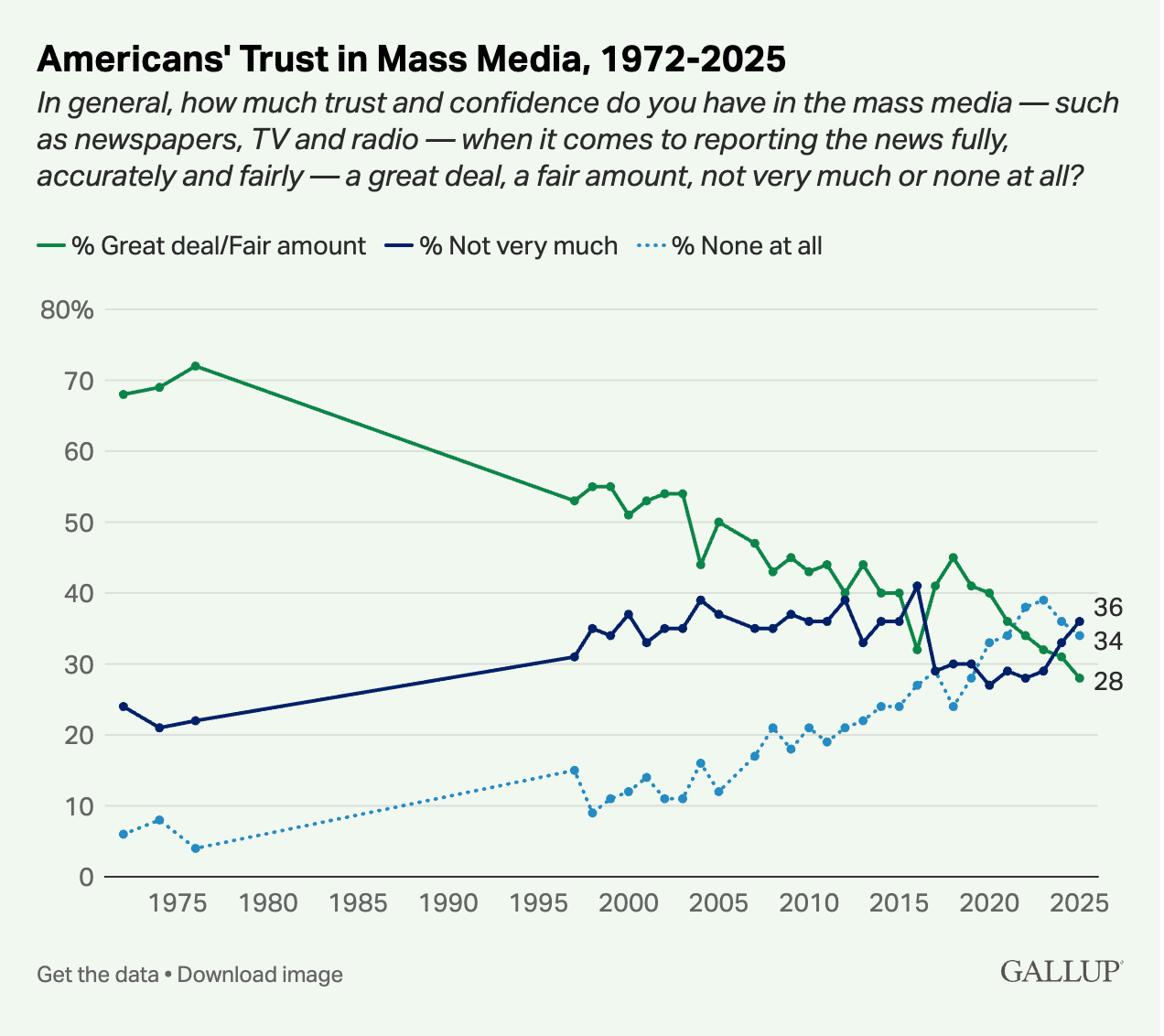
One of the things that aggravates me the most about the times in which we now live is that one can’t get an unbiased report about anything controversial from the mainstream media. There have always been newspapers that leaned right and those that leaned left, but they left all their leanings on their editorial and opinion pages. You could get a halfway decent take on anything else as it was reported legitimately in the straight-up news.
Now everything goes through political screening before being reported. The papers are suffering as a consequence, because they’re beholden to their subscribers who want to read what jibes with their politics. But it has ended up destroying the credibility of the papers involved. A truly sad state of affairs.
A new Gallup poll came out showing trust in the US media at an all time low of 28 percent.
When RFK came out with the announcement that Tylenol might be a causative factor in autism, every mainstream show and all of the left-leaning papers came out with their handpicked experts poo-poohing the whole idea. It was a knee-jerk reflex.
When I tried to see what I could find out about the subject, the only piece I found was in the Daily Caller, which is an online news site that leans to the right. The problem is, those who lean to the right will probably accept what the article says, whereas those on the left will say, Oh, it’s the Daily Caller, what would you expect them to say?
In the old days, both the NYTimes and the WSJ would have covered it, and both would have had experts from all sides. Says the Daily Caller:
The pharmaceutical company behind Tylenol privately acknowledged the likelihood of an association between its drug in pregnancy and neurodevelopmental disorders like autism in children seven years ago, company documents obtained by the Daily Caller News Foundation show.
“The weight of the evidence is starting to feel heavy to me,” said Rachel Weinstein, U.S. director of epidemiology for Janssen, the pharmaceutical arm of Johnson & Johnson, in 2018. Johnson & Johnson marketed Tylenol at the time but in 2023 spun off its consumer products division into a separate company called Kenvue.
A decade before Weinstein’s email, in 2008, Johnson & Johnson began receiving queries from consumers and physicians about a possible link, emails show.
“Not much choice but to consider this a safety signal that needs to be evaluated,” J&J Office of Consumer Medical Safety Lead Andre Mann wrote in 2008 after receiving a letter from a physician with concerns.
A 2018 internal presentation the company labeled “privileged and confidential” acknowledges that observational studies show a “somewhat consistent” association between prenatal exposure to Tylenol and neurodevelopmental disorders. Another presentation slide acknowledges that larger meta-analyses — reviews summarizing multiple scientific studies — found an association, but notes weaknesses of these studies like confounding variables and subjectivity in measuring autistic traits.
“Johnson & Johnson divested its consumer health business years ago, and all rights and liabilities associated with the sale of its over-the-counter products, including Tylenol (acetaminophen), are owned by Kenvue,” a Johnson & Johnson spokesman said in a statement. [My bold]
I wonder if as part of their due diligence Kenvue looked at the autism data? I wonder of J&J made it available?
In digging a little deeper on this, I came across a Harvard paper from just a month ago showing Tylenol caused an increase risk of autism.
When children are exposed to acetaminophen—also known by the brand name Tylenol or as paracetamol—during pregnancy, they may be more likely to develop neurodevelopmental disorders (NDDs) including autism and ADHD, according to a new study.
The study was published August 14 in BMC Environmental Health. Andrea Baccarelli, dean of the faculty at Harvard T.H. Chan School of Public Health and professor of environmental health, was senior author. The study was led by the Icahn School of Medicine at Mount Sinai and also included co-authors from other institutions.
The researchers analyzed results from 46 previous studies worldwide that investigated the potential link between prenatal acetaminophen use and subsequent NDDs in children. The researchers used the Navigation Guide Systematic Review methodology—a gold-standard framework for synthesizing and evaluating environmental health data—which enabled them to conduct a rigorous, comprehensive analysis that supported evidence of an association between acetaminophen exposure during pregnancy and increased incidence of NDDs.
And I stumbled across this X/Twitter video detailing a number of studies going back through the years in which Tylenol was fingered as a driving factor in the development of autism. For some reason, the platform I’m using or X/Twitter would not let me insert this video. I couldn’t even get the link to it to work. I don’t know if they don’t want it to be seen or what (?) because I haven’t had any trouble embedding other X/Twitter videos. So I came up with something clever that does appear to work. I’m embedding it in the link below. Click there, and you’ll be taken to X/Twitter to get the video. You’ll have to turn on the sound. I couldn’t get it to come on without doing it manually.
I am still of the opinion that Tylenol is not the prime driver of autism. I’ve read all kinds of people who should know better to write it off to genetics. There are no genetics diseases I know of that grow at the rate autism has grown over the past 50 years. That’s just not even feasible.
I think there is another factor, and, if push came to shove, and I had to bet a lot of money on it, I would bet on the childhood vaccine schedule. Autism was rare until the jabs started multiplying, then it started multiplying tool. (But of course that also conveniently coincides with the Reyes’ syndrome scare and the wholesale move to Tylenol as the febrile prescriptive of choice for pregnant moms and kids.)
Since 1986 when the companies making vaccines no longer had any liability, they did not have to worry about safety problems or even issuing warnings. If Pfizer, or any other drug company, develops any other kind of drug, they go all out on making it as safe as possible and warning those who might take it of serious side effects. Because they have to.
Chemotherapeutic drugs are a case in point. Companies that make them work as hard as they can to make them safe to take. But the nature of these drugs make them hard on many people. A large percentage have horrible side effects from them that include everything imaginable, right up to death. But the drug companies work as hard as they can to make them as safe as they can, and they issue all kinds of warnings of known adverse events.
This is why they can sell these dangerous drugs and not get sued every time anyone has an untoward reaction. They disclose all of these terrible dangers to the patients. Then the patients are informed as to what they could be in for, and they make the decision whether to go along with it or not. If they take the drug—and some of the chemotherapeutic drugs cost many thousands of dollars per week—and they have a horrid reaction, or even die, well, they’ve been warned.
It’s not like that with vaccines. With vaccines, the impetus is to get them approved. Once approved, the drug company has zero liability whatever happens to the patients. Most patients are babies or little kids, who have no choice in the matter. Most doctors don’t explain the adverse issues that can happen with vaccines. There isn’t much explanation at all—it’s just okay, time for his shots; here we go. There’ll be a little sting.
I really urge people to read Aaron Siri’s book Vaccines, Amen to understand how the vaccination business works. You’ll never look at them the same again.
I read Dr. Maryanne Demasi’s excellent Substack a couple of days ago about Trump’s press conference where Tylenol as a possible driver of autism was announced.
But he also announced that he wanted to remove aluminum from vaccines as well, which no one really challenged.
If carried through, this pledge would shake the foundations of modern vaccinology. Aluminium adjuvants have been the backbone of vaccines for nearly a century, used in billions of doses worldwide.
Stripping them out would not only disrupt a multi-billion-dollar industry but force a fundamental re-examination of how vaccines are made and tested.
The resistance would be fierce.
To understand the implications, I turned to the scientist who has spent nearly forty years warning about the dangers of aluminium in human health: Dr Chris Exley.
Known as “Mr Aluminium,” Exley has published over 200 peer-reviewed papers on the subject, showing how aluminium accumulates in the brain, how it is trafficked by immune cells, and how it may be implicated in conditions from Alzheimer’s disease to autism.
You’ll notice that aluminum is spelled and pronounced differently in the UK and, I’m assuming, Australia from where Dr. Demasi hails. Over there they call it al-u-mini-um, where as we just call it aluminum, leaving out the last “i.“
Dr Demasi has a long and excellent interview with Dr. Exley, but it is behind her paywall. I learned a lot from the interview, but want to learn more. In all the reading I’ve done about vaccines developed and used over the last hundred years, aluminum, which is not a normal inhabitant of the human body, has been used as an adjuvant for vaccines to make them work better. Since the aluminum isn’t a chemical found in humans, it’s presence stirs up inflammation and supposedly makes the vaccines work better. But at the price of having a foreign chemical roaming around in your innards. What could go wrong? A lot, apparently.
I went ahead and grabbed a copy of Dr. Exley’s book, so I could fill in the one void I have with vaccines.
His book is titled Imagine You Are an Aluminium Atom. Grab a copy and read it along with me. Something tells me that aluminum—or al-u-mini-um—is probably a much more forceful driver of autism than Tylenol.
Speaking of Tylenol… If you have a child with a fever that’s running 102F or 103F, you can bath him/her in tepid (not cold) water to break the fever. It doesn’t always work, but it does most of the time. That’s what we did with our kids. Use a glass and pour water over them in the tub or basin, including pouring over their heads. The head radiates a large percentage of the body’s heat, so you need to be sure to include it in the dousing. They’ll be miserable, but it generally breaks the fever. Without the need of Tylenol.
If You’re a Non-Diabetic, A Continuous Glucose Monitor Might Not Do You A Lot Of Good
Continuous glucose monitors (CGM) are all the rage these days, especially since they can now be had without a prescription for about $100 per month.
I wrote about them a bit when MD and I tried them a few years ago. It’s definitely an interesting experience wearing one, because you want to test all kinds of foods to see what runs your blood sugar up. You’ll find that some things you figured would send your sugar through the roof don’t do much at all, while other foods thought to be not particularly sweet drove your sugar high as a kite.
I discovered that sushi rice ran my sugar to the top in a trice. A bowl of ice cream would barely budge it. Same with potatoes, which I don’t particularly like. They didn’t cause much of a glucose change.
One day, MD and I decided to try some oatmeal. We went out and bought the expensive kind that comes from Scotland in a can and is advertised as steel cut oats.
We cooked it per the instructions in water until it thickened up, which takes a good while. We added some butter to it and a little half and half. We both ate a bowl expecting our blood sugars not to rise much. Instead, both our blood sugars went up to over 130 mg/dl and stayed up for almost two hours. When I tried the sushi rice, it raced up to about 130, but came back down almost immediately.
Delicious though they are, I’ve never eaten steel cut oats again.
CGMs are fun to play around with, but are they worth the expense? Do they make us subconsciously eat less because we know we’re wearing them?
Well, not according to one I study I came across.
The study involved 9,675 subjects who were non-diabetic had HbA1c values between 5.0% and 5.9%. As we all know, the lower the HbA1c values, the better the blood sugar control over time. Subjects were split into three groups (I don’t know how the randomization was done as this was a minimalist study.) One group wore the CGM all the time. The second group monitored intermittently using a blood sugar monitor and strips (poor bastards). The third group didn’t get squat. No CMGs; no glucose monitor or strips.
This didn’t-get-squat-bunch, of course, had their HgAic levels checked at the beginning, then at 6 and 18 months to look for changes.
Those who wore the CGM had their average HgbA1c rise from 5.49% to 5.50%.
Those who checked with glucose monitors and test strips found their average HgAic rise from 5:55% to 5.62%.
And those who didn’t do diddly as to checking had their average HgAic rise from 5.55% to 5.57%.
Here it all is shown graphically.
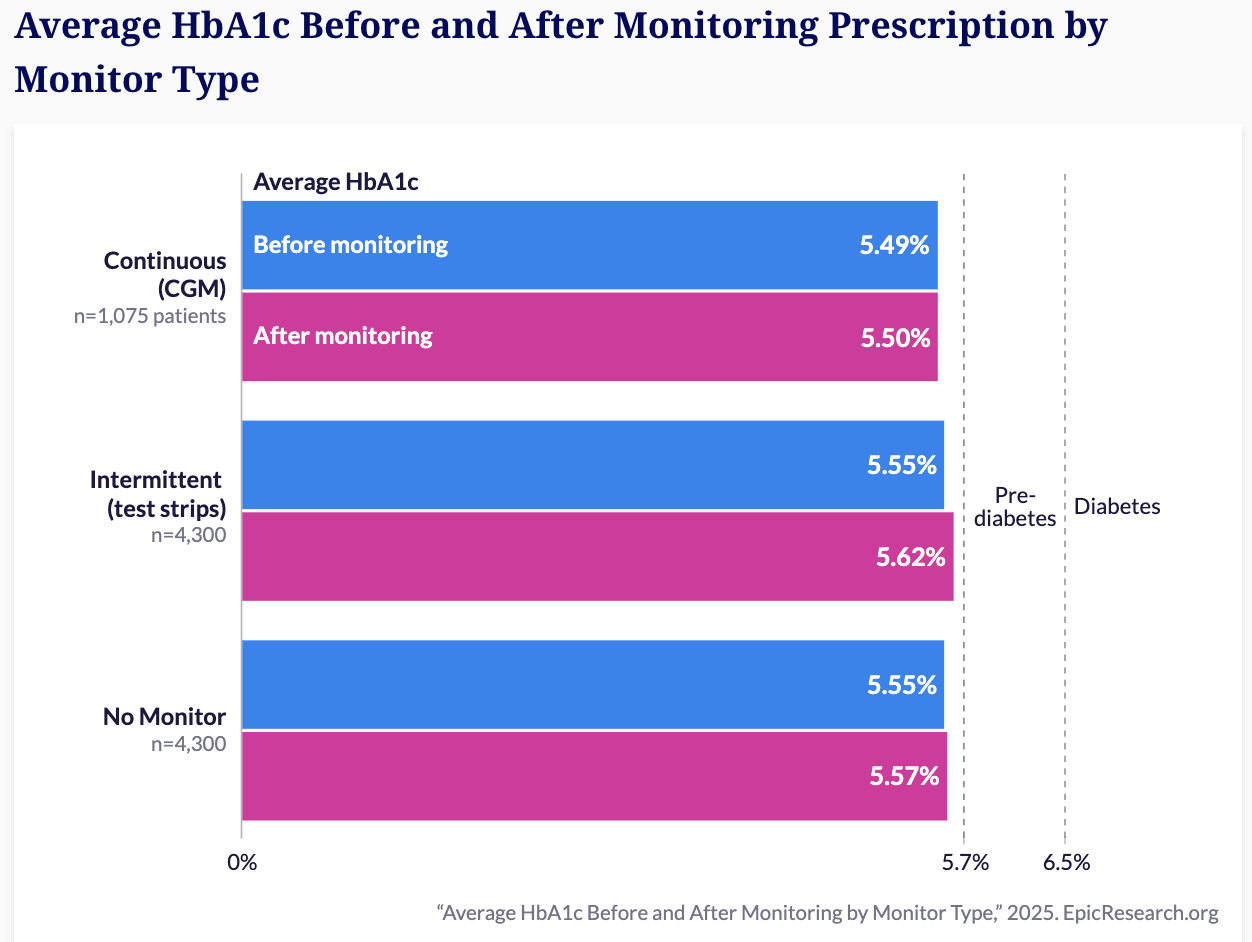
I would not say this study set the world on fire. The subjects using the CGM had a tiny (if you could even call it that) improvement over the other two groups. But not enough I would think to justify paying $100 per month on a CGM.
I suspect that those who wore the CGM probably watched it for a week or so, and maybe found the foods that causes serious glucose rises and eliminated them, but I would have suspected a larger change.
When MD and I did our experiment, we got the Libre Freestyle monitor. But we got them via prescription. I don’t know what kind are available now without a prescription. The only one I could find on Amazon was the Defcon, which I think is the only one over the counter without a prescription. It gives you 30 days of round-the-clock monitoring and will certainly tell you if something really runs your blood sugar up.
What we need is a continuous insulin monitor, but those, I fear, are a long way away. I worry that the ice cream I ate that barely budged my blood sugar was running my insulin sky high.
For what it’s worth, I would say it’s useful to give a CGM a try for a month just to see what various kinds of foods do to your blood sugar. Once you know, there is really no point in wearing one all the time.
Those with diabetes are a different story. I’m talking about non-diabetics.
Ketogenic Diets Are Helpful Against Major Depressive Disorders in College Students
When I read Georgia Ede’s great book a few years ago, I learned a lot about how keto diets worked to treat bipolar disorder and other major affective disorders in adults. Some of her stories were almost unbelievable.
Now comes a new study from Transactional Psychiatry about 24 students (10 women, 6 men, mean age 24 y/o) who underwent ketogenic diet therapy for at least ten weeks and gained a 70 percent reduction of their depressive symptoms, increased their well-being, body composition, and cognition.
The study was prompted by the ever-rising prevalence of major depression, particularly on college campuses. Typical treatments, such as psychotherapy and medication, are effective for many but don’t help everyone and can come with unwanted side effects. Researchers at The Ohio State University sought to take a different approach, one that addresses the potential link between metabolic health and depression.
A growing body of evidence connects issues such as insulin resistance and excess body fat to an increased risk of depression. The team members thought that perhaps a dietary intervention known to reduce inflammation and improve metabolic health may well improve the symptoms these students were suffering, despite already being treated for depression.
Researchers recruited students who had been diagnosed with Major Depressive Disorders, and who were then engaged in counseling and were taking medications. The study was not randomized. It was just a basic pilot study to see if enough of the students improved sufficiently to justify a larger study. All of the students were on basically the same dietary regimen.
Prior to baseline testing (BL), a dietary education session was provided to ensure participants understood the guiding principles to a WFKD [well formulated ketogenic diet] and were comfortable with adhering to the diet for 10–12 weeks. The diet intervention began after the baseline testing visit. Participants received extensive personalized education and ongoing support from the dietetic team to achieve the nutritional goals of a WFKD. The intensity of coaching varied across participants depending on their baseline knowledge and individual situation. We utilized a HIPAA-compliant messaging app (Healthie, New York, NY, USA) that allowed the participant to communicate with dietetic staff throughout the intervention. We provided staple ketogenic-friendly food items to partially offset participant food costs, ensure nutrient quality, and facilitate adherence. Ten pre-packaged ketogenic meals (Factor 75, Aurora, IL, USA) were provided to each participant at baseline to provide a visual guide of how a balanced WFKD meal should be composed for the duration of the study when participants implemented the diet thereafter at home. Subsequently, participants chose food and meals on their own with the exception that we provided a few shelf-stable items such as high-quality fats (e.g., olive oil), salad dressings, salmon & sardine packets, beef jerky, Whisps cheese crips, nuts and seeds, and an oatmeal alternative.
Throughout the study, researchers tracked several outcomes. Participants self-reported their depressive symptoms bi-weekly using the Patient Health Questionnaire-9. A qualified clinician also rated their depression at the start, midpoint, and end of the study using the Hamilton Rating Scale of Depression. To confirm they were following the diet, students measured their morning blood ketone and glucose levels daily. Researchers also assessed body composition using scans, collected blood samples to analyze for markers related to metabolism and inflammation, and administered a battery of cognitive tests on an iPad.
The results showed a robust and sustained decrease in depression symptoms. Among the 16 students who completed the study, self-reported depression scores dropped by an average of 69 percent from the beginning to the end of the intervention. Clinician-rated scores showed a similar 71 percent reduction. Every participant who completed the study showed an improvement in their depression scores, and by the end, no one met the criteria for moderate or severe depression.
Ryan Patel, a psychiatrist at Ohio State who met with the students during the trial, noted the significance of these changes. “The average effect size for medications and counseling after 12 weeks is about 50%, and we saw a substantially greater result,” he said. “That is an impressive finding, that across the board, in this real-world setting, everybody got better, and across the board, our participants did not need more treatment or emergency intervention.” [My bold]
You can see the loss in body weight in the chart below.
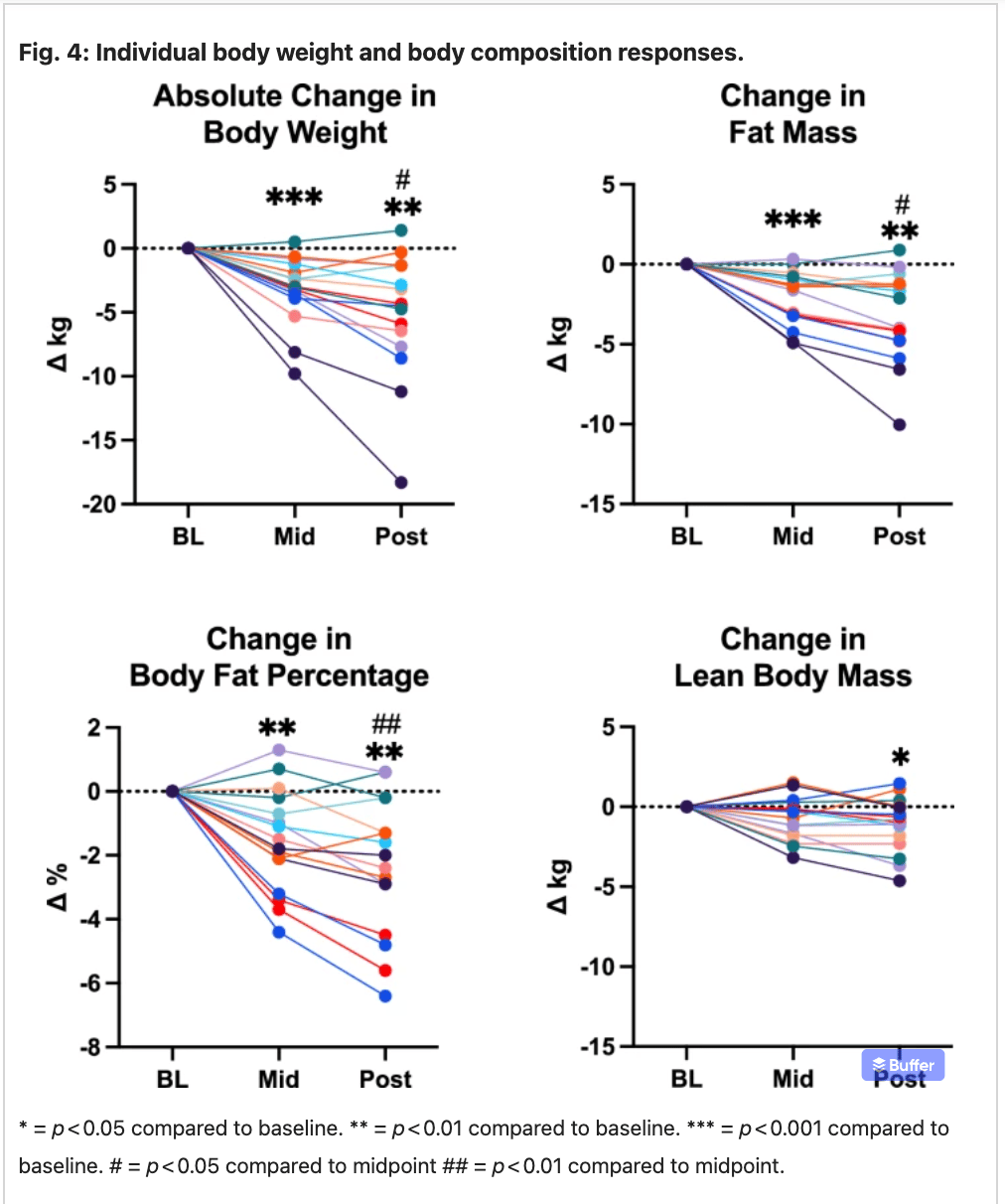
On top of weight loss, the subjects had a 32 percent growth in bone-derived neurotropic factor and a reduction in leptin. In my view, the results of this study are excellent and should prove the case for a larger, randomized trial. Many of these trials of ketogenic diets end up doing extremely well for those who follow them. Problem is, many subjects drop out because they don’t like the diet.
The researchers try to get funds for a larger study, but are denied. When asked why, they are told that the diet is excellent; it does everything it is supposed to do. But if the subjects won’t follow it, then we really don’t have a case for a larger study.
Perhaps the team on this study has figured out a way to encourage the subjects to stay on the plan. They all feel so much better and think so much better, you’d think they’d never want to go off. But in most of these studies they do. I hope this group of researchers can gather a larger patient group and come through with some real breakthroughs.
Odds and Ends
1 million-year-old skull from China holds clues to the origins of Neanderthals, Denisovans and humans.
An asteroid, with a four percent chance of hitting it, might be heading for the moon. Should we nuke it? Serious business.
Archaeologists discover a 5,000-year-old tomb in Spain filled to the brim with ancient treasures. Ah… my love of treasure hunting. Always a day late and a dollar short!
Giant trees of the Amazon get taller as forests fatten up on carbon dioxide, which makes sense since carbon dioxide is food for plants.
Can music make your food taste better? Spice up your meals with some sonic seasoning.
Built by gaming veterans, this Dallas AR startup Is reanimating the past to own the future of tourism.
The mechanisms driving the meters-higher sea levels a few thousand years ago do not support claims that CO2 is a driver.
Archaeologists discover life-sized animal carvings etched into Arabian desert rocks between 12,800 and 11,400 years ago, revealing human activity in the arid desert roughly 2,000 years earlier than previously thought.
Known to some as the “Freshwater Everest, there is a huge mountain completely submerged in the middle of Lake Superior.
Notre Dame reopens its towers and rooftop. I remember climbing up there to hang out among the gargoyles as a broke college student on a summer trek through Europe on $5 a day.
5 words that meant something completely different 50 years ago. (Or in some cases, since I was actually there 50 years ago, really didn't.) If, like me, you had reached your majority and a few more 50 years ago, you'll laugh at some of these.
Scientists and archeologists team up with modern technology to create a digital 3D mapping of Pompeii. Fascinating video documentary on the work being done.
A group of historians and citizen scientists (the best kind) find shipwreck lost for 139 years in Lake Michigan and it just took them two hours.
3000 year old Egyptian bracelet stolen, sold, and smelted. What an unspeakable loss; what a tragedy. I hope they throw the book at the perps.
How 10% of a tiny town in Quebec became multi-millionaires. Always the bridesmaid!
The first two traffic tickets I ever received were for jaywalking. Why do we call it that?
Pick an era and listen to the music from it. It's a real rabbit hole, I warn you, but ah, the nostalgia.
How a massive civil engineering project rendered Disney World nearly mosquito-less, even though it was plopped smack in the middle of Florida swampland. And in my view, there’s no greater service than to render anyplace (even the biggest people trap ever built by a mouse) mosquito-free!
75-year-old female power lifter heads to the world championships. And from my birth state no less. Yes, fellow goobers, it can still be done! (Just click the little blue down arrow on the right of their screen to escape being asked to subscribe.)
Organization and activity lead to longevity, study finds. And here I always thought a clean desk was the product of a sick mind. Or so I told myself amid the clutter and piles of books on my desk and nightstand.

Video of the Week
Okay, you know from the first part that you’re in for a bit more of Roger Miller. But this one was unexpected for us. MD and I traveled a fair amount with the kids, so though they grew up in Arkansas, and had traveled a lot and had been to a lot of big cities, it was probably their first time to the Big Apple.
When we got there and got seated at the Eugene O'Neill Theatre we had no idea what we were in for. We hadn’t heard the sound track, so we were clueless. We just knew it was a Broadway Musical version of Huckleberry Finn with a score by Roger Miller.
We loved the show and near the end—totally unexpected by us—was this song. I can’t find it in the Broadway version, but I did find on sung by Roger Miller himself.
Imagine our surprise when our little family of five heard this in the Big Apple.
Time for the poll, so you can grade my performance this week.
How did I do on this week's Arrow? |
That’s about it for this week. Keep in good cheer, and I’ll be back next Thursday.
Please help me out by clicking the Like button, assuming, of course, that you like it.
This newsletter is for informational and educational purposes only. It is not, nor is it intended to be, a substitute for professional medical advice, diagnosis, or treatment and should never be relied upon for specific medical advice.
Thanks for reading all the way to the end. Really, thanks. If you got something out of it, please consider becoming a paid subscriber if you aren’t yet. I would really appreciate it.
Finally, don’t forget to take a look at what our kind sponsors have to offer. HLTH Code, Precision Health Reports, and Jaquish Biomedical.
And don’t forget my newest affiliate sponsor Lumen. Highly recommended to determine whether you’re burning fat or burning carbs.
Reply