- The Arrow
- Posts
- The Arrow #250
The Arrow #250
Michael Eades
October 16, 2025
Greetings everyone.
I’m going to start off this week’s Arrow in a sort of blind rage. I’ve been so busy with all kinds of issues the last couple of weeks that I’m behind in everything, it seems. I’m woefully behind in emails, tab removals, and I’m especially behind in my reading, which I almost never neglect.
When it came out a few weeks ago, I immediately purchased Aaron Siri’s book Vaccines, Amen despite its kind of weird title. I bought it in Kindle, which is how I do most of my reading these days, because I travel so much it makes schlepping a thousand books as easy as schlepping one. What one does not realize about Kindle books, however, is how long some of them are. There is a little percentage number that pops up on the bottom right showing the percentage of the book in question that has been read.
I’ve been reading and reading and reading on Siri’s book, and I just noticed a day or two ago that I’m not even halfway through it. I usually whip through a normal book fairly quickly, but I still have miles to go with this one.
Fortunately, the book is engrossing, so it keeps me going despite my time restrictions of late. Not only is it engrossing, it is infuriating, so I’m asking you to indulge me and just let me get some of the pent-up fury out of my system.
I’ve purchased just about every book on vaccines I’ve come across since the start of Covid when my interest was really piqued for the first time. I bought all of the books—there were three of them—extolling the virtues of the new mRNA vaccines and describing how they were made. From there, I moved on to Dissolving Illusions and Turtles All the Way Down, both of which proved to be real awakenings for me.
Over this past week, I read somewhere that doctors get only one week of study on vaccines during medical school. I was a diligent attender of classes in medical school, and, for the life of me, I can’t think of a single lecture we had on the subject, other perhaps than being told a few existed (polio, smallpox, tetanus) and they were all good. Nothing about their scientific validation. Of course, I was in medical school in the late 1970s, which was before the 1986 law indemnifying vaccine makers and opening the floodgates to vaccine development.
I’ve been looking for a book describing in detail all the vaccines and the testing they each went through before being used on babies and children. Siri’s books does that very thing starting a little before halfway through. Which is what has me so riled up.
I’m going to quote extensively about one vaccine, because it puts it all in perspective. But realize that all vaccines are essentially the same in terms of the shoddy testing. No other drugs can I think of have ever had such an easy route to approval. Most drugs are made for adults, but vaccines are made primarily for children, who have little to no choice as to whether to take them or not.
Before I get into what’s got me so fired up, I want to write a little bit about doctors and lawyers and the difference between them.
Doctors, Lawyers, and the Legal System
When I downloaded Siri’s book from Amazon, I gave myself a warning: He’s a lawyer; be careful. I had seen YouTubes of Siri disemboweling doctors (a number of which I have posted in the Arrow), who seriously needed public disembowelment. But I always try to keep the differences between doctors and lawyers in front of mind. There is a big difference between the two.
Doctors and lawyers have vastly different goals. Even the most incompetent doctors, I believe, truly want to help their patients. Lawyers want to win cases.
I’ve had the pleasure to know two outstanding lawyers (neither of which has ever sued or deposed me, thank God), from whom I’ve heard countless war stories. When lawyers take a case, they usually base it on some legal theory. If, as the discovery rolls in, they find their theory is not going to work, that something blew up, they don’t just say, Okay, well, we spent all this time and money taking us to this point, but the facts about the guy (company, whatever) we’re suing don’t fit with our theory, so we’re just going to let him off the hook.
Not a chance. They go in search of a different legal theory that may work with the new info they’ve discovered.
When doctors take care of patients, they get paid irrespective of outcome. When plaintiff’s lawyers take a case, they end up fronting all the money for the case (unless, of course, their client has deep pockets) which often isn’t the situation. They get paid only if and when they win. And even then it can take forever as things go through appeals.
Aaron Siri is a plaintiff’s attorney. He wants to win. So, I warned myself to be careful as I read his book, and to make sure I checked all the references to ensure what he was saying matched the documentation. I spot checked here and there, and everything held up. But for what I’m about to show you, the part that has me so troubled, I checked everything.
If you put a lawyer up against a doctor on a medical matter, who do you think is going to win?
I can tell you, it’s almost always the lawyer. Why? Because the doctor typically thinks he knows everything, so doesn’t bother reviewing before the encounter. The lawyer, on the other hand, does know everything, because he’s spent hours pouring over documents and learning all the intricacies of what the case is about.
Which is why you’ve seen all these doctors have their asses handed to them by Siri in the YouTubes I’ve posted.
The classic is the deposition of Stanley Plotkin, M.D., the high priest of vaccinators, the author of Plotkin’s Vaccines, the standard textbook on the subject, and the mentor and trainer of all the pro-vaccine doctors out there screaming that vaccines are harmless. (Think Paul Offit.)
Plotkin waltzed into his deposition figuring he knew everything there was to know about vaccines, because, after all, he is Stanley By God Plotkin. Siri made him pay. It’s fun to watch. If you want to see the entire thing, you can find it here.
Remember as you watch that this is the top vaccine expert in the world.
Now let’s get to what has me so worked up.
First, Siri describes what a serious adverse even is as defined by the FDA.
Death
Life-Threatening
Hospitalization
Disability or Permanent Damage
Congenital Anomaly/Birth Defect
Required Intervention to Prevent Permanent Impairment or Damage
Other Serious (important Medical Events) (…the event may jeopardize the patient and may require medical or surgical intervention…to prevent one of the other outcomes.)
The vaccine I want to discuss is the Pneumococcal (PCV) vaccine, which is injected into children at 2,4,6, and 12 months of age. If they follow the schedule, they get it four times.
I’m going to quote liberally from Siri from this point on, because the whole thing is so outrageous that it beggars belief. As you read what Siri has to say, remember the list above of what the FDA defines as serious adverse events.
The first PCV ever licensed for children in the United States was Prevnar 7 in 2000. Despite the fact it was the very first one ever licensed, the clinical trial to license this vaccine did not use a placebo. It could have used a placebo, but it didn’t. Instead, and this is going to sound unbelievable, the control was another unlicensed experimental vaccine. Literally, it was “an investigational meningococcal group C conjugate vaccine [MnCC],” meaning an unlicensed experimental vaccine. Let me repeat that: Prevnar 7 was licensed based on a clinical trial which compared safety to another experimental vaccine. Seriously, I couldn’t have even dreamed of making this up.
Even a group of FDA and CDC scientists conceded that comparing Prevnar 7 to a experimental vaccine means it was not possible to determine whether it was safe:
“Prior to licensure, … the control group in [Prevnar 7’s] main study received another experimental vaccine, rather than a placebo. If both vaccines provoked similar adverse events, little to no difference between the 2 groups might have been evident.”
Meaning, by FDA standards, Prevnar 7 just needed to be as safe as another experimental vaccine—which could have been a very dangerous product. That is obviously a ridiculous trial to use to determine whether Prevnar 7 was safe. And it would be funny if we were not talking about the health and safety of newborn babies.
It gets worse. In 2010, Prevnar 13 was then licensed based on a clinical trial in which Prevnar 7 was used as a control. Of course, all that means is that Prevnar 13 was as safe as Prevnar 7 which itself was licensed only because it was as safe as another experimental vaccine. While that alone is concerning, here is where it really gets concerning. In Prevnar 13’s clinical trial, the results showed: “Serious adverse events reported following vaccination in infants and toddlers occurred in 8.2% among Prevnar 13 recipients and 7.2% among Prevnar [7] recipients. [my bold]
That should have been a stunning finding. It should have been deeply concerning that, among previously healthy infants, 8.2% of Prevnar 13 recipients and 7.2% of Prevnar 7 recipients suffered a serious adverse event. As we have seen above, a “serious adverse event” means a grave harm. Instead of raising alarm bells, which this should have, Prevnar 13 was deemed “safe” by the FDA and licensed for use in babies because it had a similar serious adverse reaction rate as the control group receiving Prevnar 7. Again, safe by the FDA’s approach, not safe by any thoughtful, moral, or ethical standard.
Seriously, when 7% to 8% of previously healthy infants had a serious adverse event rate from Prevnar 7 or Prevnar 13, that finding should have caused heads to explode. No PhD is required for that to cause concern. Just common sense and a smattering of empathy. It should have made them, at the least, question the safety of both products, given that Prevnar 7 was licensed only because it was as safe as another experimental vaccine.
Amazingly, in explaining this incredibly concerning rate of serious adverse events, Pfizer (which profits from these products) stated that because the trial for Prevnar 13 reviewed safety for six months, rather than 30 days (and 60 days for hospitalization) as occurred in the trial for Prevnar 7, the high rate of serious adverse events may have been due to the longer observation period. But that is not an excuse. It is an indictment. Yet the FDA accepted this excuse.
As Pfizer’s FDA-approved package states: “This reporting period [of 6 months] is longer than the 30-day post-vaccination period used in some vaccine trials. The longer reporting period may have resulted in serious adverse events being reported in a higher percentage of subjects than for other vaccines.” Again, how in the world is this an excuse? This should be cause for real alarm and highlights the issue with short safety reviews.
Yet, instead of pausing to ensure the safety of these products after this shoddy trial showed troubling results, the pyramid scheme continued. Prevnar 13 was then used as the control to license Vaxneuvance, PCV-15, for children in 2022. In that trial, “serious adverse events…were reported by 9.6% of Vaxneuvance recipients and by 8.9% of Prevnar 13 recipients” but the new vaccine was nonetheless deemed “safe” because there were “no notable patterns or numerical imbalances between vaccination groups.” In other words, the vaccine was deemed safe by the FDA’s standard but not by any rational, thinking, or ethical standard.
In 2023, Prevnar 13 was again used as the control to license Prevnar 20, (PCV-20), for children, and this trial again showed high rates of serious events in both vaccine groups. This time, to obfuscate the concerning results, the findings were split into two categories: “serious adverse events” and “newly diagnosed chronic medical conditions.” Despite the high rate of serious harm in both vaccine groups, the FDA deemed the product “safe” because there were “no notable patterns or imbalances between vaccine groups.
In short, PCV-20 and PCV-15 were licensed using PCV-13 as the control. PCV-13 was licensed using PCV-7 as the control, and PCV-7 was licensed using another unlicensed experimental vaccine as the control. In each of these trials, the serious adverse events rate was high in both vaccine groups; but because the rate was similar in both groups, each met the FDA’s artificial standard for what it deems as “safe.”
I have been in the room with parents whose children have been seriously injured by a PCV vaccine when they learn what was relied upon to license these products. The range of emotions is heartbreaking: some break down from guilt for not having more carefully reviewed these products, while others express anger—even rage. In my experience, however, these parents remain largely unemotional toward the products themselves—unlike the Vaccines, Amen crowd. Their focus and pain relate to their injured child, whose safety was plainly not of real concern in these PCV vaccine trials.
Now do you see why I’m so pissed off?
These are little, bitty babies, our most vulnerable population, that are getting these truly not-legitimately-tested vaccines that have a serious adverse event rate of almost one in ten. And did you notice that as each new version of the PCV was developed, the serious adverse event rate went up a bit. It was still within statistical tolerance of the previous version. But if you look at the first version tested (Prevnar 7), serious adverse events occurred in 7.2% of babies vaccinated. Then in each ‘upgrade’ of the vaccine, the serious adverse event rate nudged up a little higher until we get to the latest version (PCV-20) in which the serious adverse events were split into two categories: “serious adverse events” and “newly diagnosed chronic medical conditions.” So we have no idea what the percentage of serious adverse events are.
The Siri book breaks down every vaccine on the schedule and describes how it was tested. They are essentially all the same. It’s just that the PCV went through more iterations, so I thought it would be of interest for readers to understand just how corrupt and screwed up the system is.
One last thing…
Most of the vaccine books I’ve read have nothing positive to say about any vaccine. Siri is pretty up front about which ones (very few) do have positive benefits (the DPT, for example), which all involve protecting the person who has been vaccinated. None of them prevent the spread of disease, so he asks the logical question: Why are there vaccine mandates for kids to be able to attend school? If all a given vaccine does is protect the recipient, why isn’t vaccination a personal choice? Why the forced mandates? Kids getting the vaccines to protect themselves don’t protect other kids. Even the recipient of the vaccine can spread the disease without getting it. So what is the point of forcing every kid to get vaccinated? In my view, it’s a combination of a control issue and ignorance.
If you would like to support my work, take out a premium subscription (just $6 per month).
An Inconvenient Study
Three or so weeks ago I was inundated with emails from friends and readers telling me I absolutely had to watch this film. I clicked on the link and realized it was an hour and 20 minutes long, and given all I had going on, I just couldn’t justify the time to watch it.
Plus, I had already heard of the study, which is the movie’s subject, and I knew it was a retrospective cohort study, which can’t really prove causality. That fact, too, justified my not spending the time to watch it. And I had heard some of the mainstream criticisms of the study (and movie), many of which were valid, particularly the part about this type of study not being able to prove causality.
But I finally succumbed and watched it. One of the reasons I’m predisposed not to watch films that are arguing an issue—in this case, that vaccines could well be dangerous—is that the maker(s) of the film or documentary design it to make the viewer arrive at a specific conclusion. Thus, I always feel like I’m being manipulated.
I’ve got to say that this one is obviously forcing a point of view, but near the end spends a lot more time than I would have expected discussing the reasons the study did not, and could not, prove causality. Studies like this one are basically done to see if there is any justification for doing a randomized, controlled trial, which is much more expensive, but that can come much closer to proving causality.
Problem is, where vaccines are concerned, you’re going to play hell getting an RTC done.
Why?
Because the vast majority of people believe vaccines are safe and effective. Life saving even. If you read and study as much as I have, you know that’s not true. But most people just follow the recommendations of their pediatrician, which could well end up crippling their kid for life. And once harmed, there is no going back. No do-overs.
The common perception that vaccines are essentially harmless and lifesaving bolsters Big Pharma’s claim that it would be immoral and unethical to deny a child a vaccine by randomizing it into a control group. You might think that many parents who are suspicious of vaccines might volunteer to have their child in a control group. But that wouldn’t work, either.
Why?
Because a randomized study has to be a randomized study. Both groups have to be the same. And parents of children who are educated on the perils of vaccines may be way different than parents who are happy to have their kids get every vaccine that comes down the pike. (That would have been my own mother, bless her heart. All I can say is thank God there were but a few vaccines when I was a child, because had there been 50, I would have gotten them all.)
Parents who are knowledgeable about the dangers of vaccines may have many child-rearing practices that are different from those like my mother. They may not let their kids drink soda or eat junk. They may encourage more outdoor play. Or not. The two groups of kids would be different if people could simply volunteer for the control group.
As long as Big Pharma can propagandize how unethical it would be to deny children a vaccine, the closest thing we’re going to get to an RCT is the PCV experience I wrote about at the start. The control group will get an older vaccine, which was itself never controlled against placebo, so it’s really not an RCT at all.
I had (have) great hopes that RFK will to try to push RCTs for vaccines through, but I’m beginning to believe the money from Big Pharma is just too much for him to overcome. Think of all the people in congress who are getting funded by Big Pharma. I suspect the majority of them are getting some funding.
If Trump lets RFK run wild, then he (Trump) will be besieged by GOP congress people on the Big Pharma dole whining to him that they are in a close race in 2026, and if they don’t have Big Pharma support, they will likely lose. If enough of them lose, then the GOP loses the house, and the first thing that will happen if the Dems take over is that they will start impeachment proceedings against Trump. He’s already had it happen twice. Plus, with a divided congress, he’ll never get anything passed. So, I’m sure it’s a sobering prospect for The Donald. As it would be on the other side of the political aisle were the situation reversed.
One of the reasons I’m pretty certain something is going on was the announcement that Trump had his annual physical just before he left for Israel. And, along with his physical, it was announced that he had both a Covid booster and a flu shot, two of the most useless vaccines out there. The data is clear that the more Covid boosters one gets, the more likely one is to get Covid. And flu shots protect (if they even do that) against last year’s flu, while at the same time predisposing those who get it to come down with more non-influenza upper respiratory illnesses than those who don’t.
(My opinion is that Trump didn’t take either shot, but that’s just my opinion. I have no knowledge one way or the other.)
Why would they announce Trump had taken these shots unless Big Pharma had a hand in it?
And now, a word from our featured sponsor… please check out their products if you need to focus better during the day, chill, relieve stress, and get a good night’s sleep to be ready for tomorrow.
Protein, Protein, Protein
I’ve written often in these pages about the issues with GLP-1 agonists and protein intake. Basically, what these drugs do is to prevent or at least decrease hunger. If you aren’t hungry, you probably won’t eat. So the GLP-1 drugs end up putting you on a low-calorie diet that doesn’t make you hungry all the time.
Most low-calorie diets restrict food, and thus end up restricting protein. If you’re not particularly hungry, you’ll more often than not tend to eat carbs. Protein, which in real life is almost always found in combination with fat, is not as appealing appetite-wise as, say, a brownie. And if you’re losing weight anyway because of the effects of the drug, what the hell. Go for the brownie.
As a consequence, the studies on GLP-1 agonists all pretty much show that somewhere around 40-45 percent of the weight lost is muscle mass (and other protein structures). I’ve discussed ad infinitum in these pages how difficult it is to regain lost muscle mass. The older one gets, the more difficulty one has in rebuilding muscle mass, so the loss of 40 percent is pretty critical.
This has received enough news coverage, I suppose, that the purveyors of UPF junk food are trying to jump on the protein bandwagon now.
I happened to see this ad when I was trying to catch the last inning of the baseball playoffs.
Not only did I see the ad once, I saw it yet again before the game was over. And I watched only the last inning.
If you take a look at the nutritional label of these instant oats, you’ll find that most of the protein is provided by whey protein concentrate and a tiny bit of whey protein isolate. With a bit coming from the oats and the almonds.
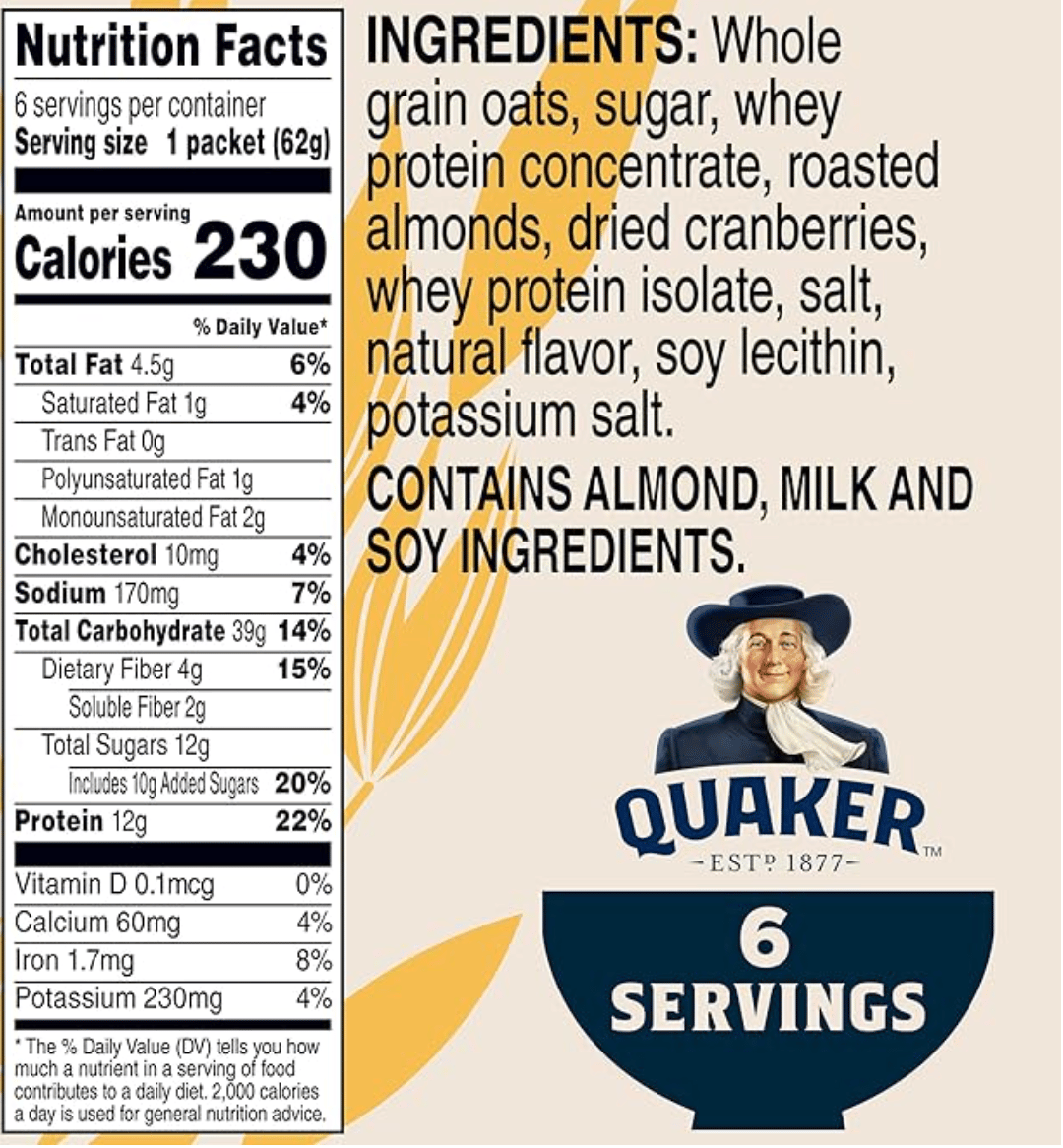
Ingredients are always ranked on a label from most plentiful to least. As you can see, both the whey protein concentrate and the whey protein isolate are lower on the ingredient list than the sugar content. Which is, as you might imagine, no bueno.
Let’s look at the protein.
Whey protein concentrate is basically dehydrated whey. It is what’s left over after the curds have been removed from milk, and it’s been dried out. So it contains some lactose (thus the milk mention above) and some fat. Typically, whey protein concentrate has about 18 g of protein per ounce. Whey protein isolate is a more processed product, that is basically all whey protein, so mostly free of lactose and fats. It weighs in at about 23 g protein per ounce.
As you can see from the above label, the whey protein concentrate is near the top while the whey protein isolate is near the bottom. Which means there is a lot more of the former than the latter.
To give the Quaker Oats people some credit, whey protein is a complete protein, so I suspect this product is going to be better for you than if it didn’t have the added grams of protein.
I tried to look up Quaker Instant Oatmeal (without the extra protein), and it was nowhere to be found. The closest I could come was Quaker 1-Minute Oats, which is pretty instant. Here is the product label.
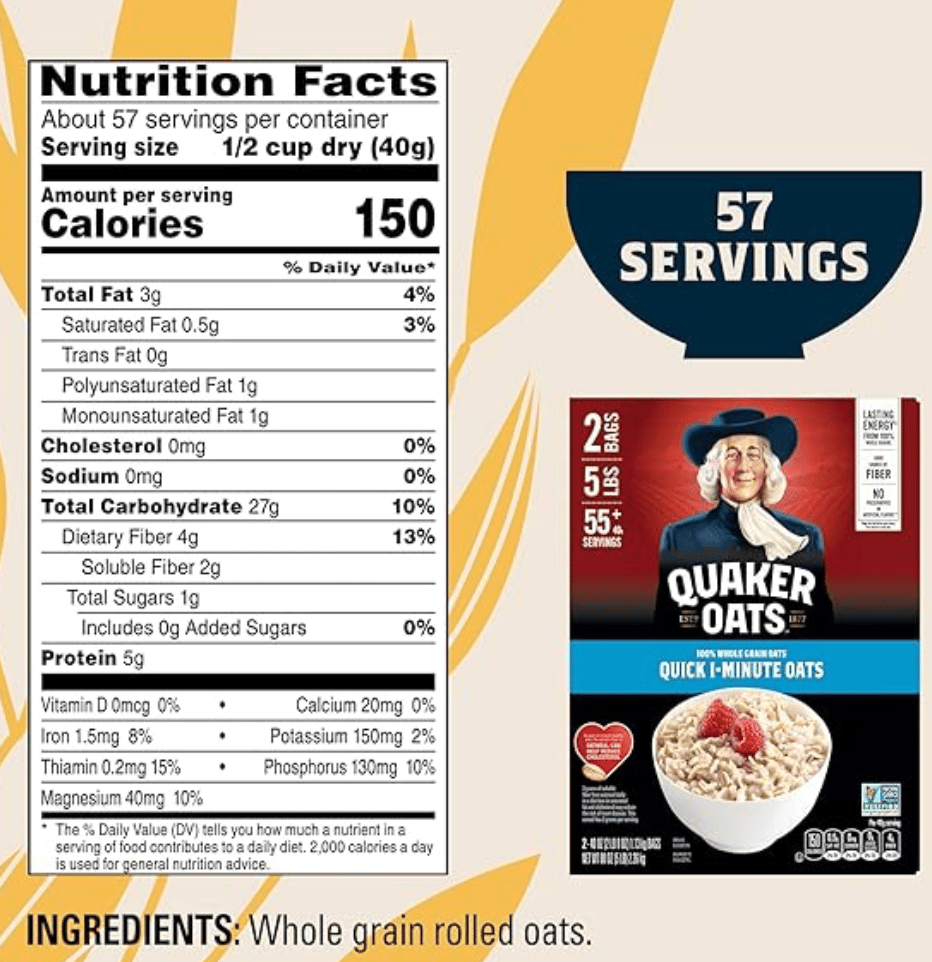
As you can see, these oats contain only 5 g of protein. But they also contain 27 g of carbs vs 39 g in the high-protein version. The 1-minute oats contain only 1 g of sugar whereas the high-protein version has 12 g. Pretty big difference.
I suspect they had to hide the taste of the whey protein somehow, although it isn’t especially unpleasant, or maybe to alter the mouthfeel. Whatever the reason, they elected to use added sugar to do so. You get 7 more g of protein in the high-protein variety as compared to the 1-minute oats, but you also get an extra 11 g of sugar. Probably not a good tradeoff. Just the oats by themselves will skyrocket blood sugar if my experience is any guide. You sure don’t need 11 g more of pure sucrose to add to the equation.
Seeing this ad on TV made me wonder if there were other products jumping on the protein bandwagon. Sure enough, a little googling brought me a real beaut. MSN reproduced a Bloomberg article (allowing us all to read it, since those are usually behind paywalls) on how many food companies are surging headlong into added protein.
The article was accompanied by an absolutely hideous video about Pop-Tarts, which I saved for your viewing enjoyment. When I pulled it up today, I discovered that the videos were on some kind of reel, and when I tried to find the one in the article when I originally read it, I realized it might take me most of my natural life before it came up in the queue again.
Not to worry, however, as I found it on YouTube, so you can be as disgusted as I was in watching it.
But first the article titled Protein Is Showing Up in Doritos, Waffles and Now Even Pop-Tarts. It looks like everyone is going all in on protein.
The protein craze that turbocharged energy bars and meat sticks is now coming for sugar-frosted Pop-Tarts.
Starting in early November, pop-tart maker Kellanova will offer a version of the sprinkle-strewn toaster pastries with the kind of higher protein content reserved for what are typically considered healthier foods. This follows PepsiCo Inc.’s plans for a higher-protein version of Doritos. Elsewhere, protein is being added to popcorn, pasta, bread, cookie dough, ice cream and macaroni and cheese.
The trend shows how packaged-food companies are betting that protein can lure back shoppers who have moved away from highly processed products. Food companies say consumers are looking for some nutritional benefit even in foods that aren’t considered healthy as they try to lose weight and ward off cravings. Many users of GLP-1s are also increasing their protein intake to help retain muscle mass. [My bold]
“I don’t think we’re anywhere close to the peak” of protein demand, which has been building for years, according to Randy Burt, a managing director at AlixPartners specializing in food and beverages. “Most consumers in the US believe they need to increase their intake of protein,” he added, predicting that increasing popularity and availability of GLP-1 drugs such as Wegovy and Mounjaro would continue to fuel demand for protein. [My bold]
I don’t know as I’ve ever eaten a Pop-Tart, three billion of which were sold just last year according to the article. But reading the following paragraph will ensure that I never will (or never will again if I have actually eaten one, about which I have no memory.)
First sold in 1964, the Pop-Tart was originally called a “fruit scone,” but was quickly renamed. In 1967, the company added frosting that wouldn’t melt in the toaster and the following year, it added sprinkles. Today, there are dozens of flavors of the toaster pastries as well as Pop-Tart branded breakfast cereal and a miniature version known as “Bites.” [My bold]
Frosting that wouldn’t melt in the toaster?!?! What in God’s name did they put in it to prevent melting in a toaster, which can get really hot? I’ll pass, thanks.
Strangely enough, I could find the nutritional labels only in Spanish. The ingredients were shown both in Spanish and English. The Spanish is easy enough to read.
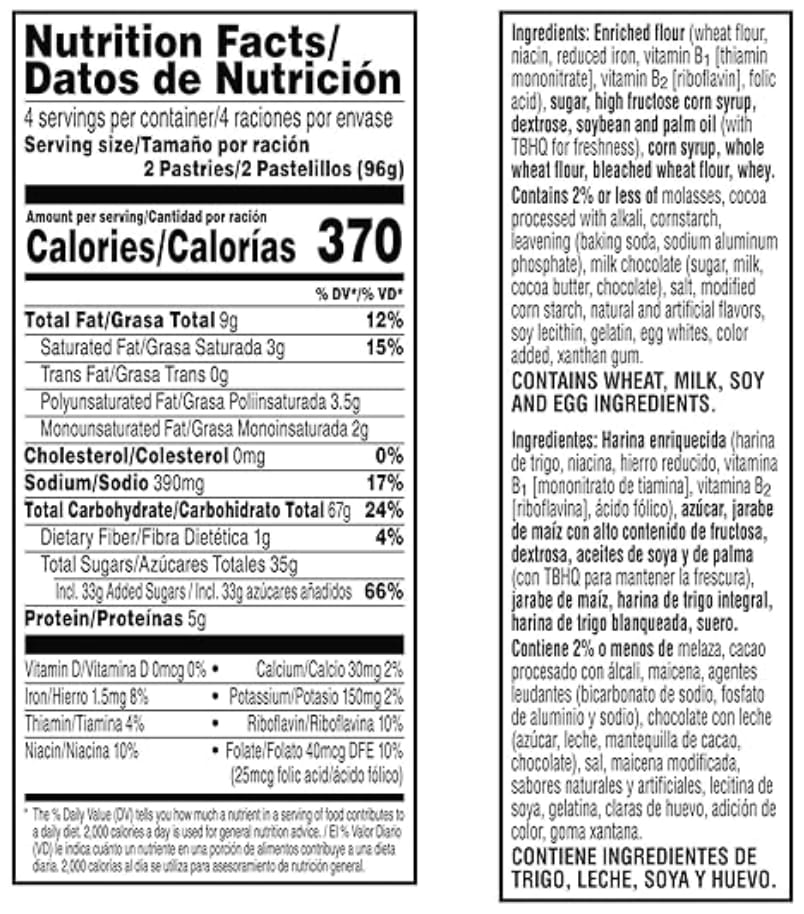
To quote Ricky Ricardo, “Ay caramba, Lucy!” It’s pretty easy to tell that there are plenty of carbs and not very much protein, but these are not the high-protein versions. Those must not be available yet. I even went to the Pop-Tarts website and couldn’t find them. Interestingly, I couldn’t find the Nutrition Facts, only the ingredients. Looking at which lets you know these are definitely ultra-processed foods by anyones definition.
According to the article
The new versions of Pop-Tarts will have 10 grams of protein per serving in three flavors: brown sugar cinnamon, strawberry and blueberry. To up the protein intake, the company is adding wheat protein concentrate and a milk protein concentrate to the dry ingredients that are used to make the toaster pastries’ dough.
The filling, frosting and sprinkles will remain the same and the pastries will overall appear very similar to their standard counterparts, though they will taste slightly different, Mccann said.
“When you add protein to things, it browns a little differently,” she said. “It creates a bit of a toasty flavor to the dough, or the crust of the Pop-Tart.”
The sugar content will be similar to regular Pop-Tarts, which have about 30 grams of sugar per serving, depending on the flavor. That’s roughly 60% of the recommended daily intake. The high-protein version will cost $3.99 for an eight-pack, compared with $3.49 for the standard pastries.
Since these products haven’t come to market yet, I’ve got a good idea for a label for them.

Okay, on to the video you’ve all been waiting for. It is truly nauseating. The narrator is either a woman with iron filings in her voice or a man. I couldn’t decide. If the latter, the less said, the better. Enjoy!
And while we’re on the subject of protein, we just learned that our online Power of Protein course is opening for enrollment in November through Adapt Your Life Academy.
Enrollment only opens once a year and will only be open for 3 days, so if you don't want to miss it, you can join the waitlist here.
In this course, you'll learn the science-based facts, not only of how important protein is in your daily diet, but also how eating the right amount of protein can help you lose weight, boost your health ,and feel fit in just weeks.
PS: When you join the waitlist, you'll get reminders via email from Adapt Your Life Academy when enrollment opens on November 18.
CICO vs Other Theories of Obesity
As you all know, the calories-in vs calories-out bunch are constantly babbling on about how obesity is caused by a simple caloric imbalance. You eat too much; you get fat. You curb your calories; you get thin. Or it can be done with exercise. Ha! Eat less, move more, and all that.
As I’m sure readers of this newsletter know, it’s all BS. It really doesn’t work that way. We may not have pinned down exactly how it does work to the finest detail, but it ain’t a caloric balance issue.
Nobel laureate Richard Feynman was a walking quote machine. Below is one of my favorite quotes of his on how science works.
It doesn't matter how beautiful your theory is, it doesn't matter how smart you are. If it doesn't agree with experiment, it's wrong.
There you have it in a nutshell. If you’ve got a pet theory, all you’ve got to do to destroy it is find a situation in which it doesn’t work. Then you can modify your theory taking into account the situation in which it doesn’t work. But every time you find a different situation in which your beautiful theory doesn’t work, then odds begin to fall in favor of your theory turning to crap.
A few days ago, while I was searching for a paper in my files. I came across an old paper by Julius Bauer, M.D. from 1947. Dr. Bauer was a Viennese physician who escaped from the Nazis in 1938 and made his way to the US. He was one of the leading researchers on obesity in Europe at the time, and he was not a believer in CICO.
Unfortunately, most of the leading American obesity researchers, the most notorious of whom was Louis Newburgh, M.D. from the University of Michigan, had bought into the CICO idea. Those physicians from Europe were kind of relegated to second class citizen status, much like those doctors are today who are skeptical of vaccines. Maybe not that bad, but close.
When I came across Bauer’s 1947 paper, I decided to search to see if I could find others. Indeed, I had in my own files a paper from 1941 that is much better and more comprehensive—in my view, at least—than the 1947 paper.
In the 1941 paper, Bauer writes
As nobody is in doubt that the law of conservation of energy holds also for the animal body and as it is an established fact that any surplus of intake of energy as compared with its output leads to accumulation of fat in the body, obesity may be called the result of an imbalance between energy intake and energy output. Such a statement is a tautology rather than an explanation of the nature of obesity.
This is precisely what those of us who are advocates of the carbohydrate-insulin model of obesity say all the time. The whole CICO scheme is a tautology. And Bauer wrote it in 1941.
What he means by this is that if one overeats enough, one will gain weight. No magic there. That’s as far as CICO takes it. Devotees of CICO try to come up with all kinds of reasons people overeat, the main one right now being the food availability situation. It’s like the old joke about being on the seafood diet. The punchline of which is, I see food; I eat it.
But there have been a number of overfeeding studies done, all of which show that when people are overfed beyond their normal diet, they don’t gain as much weight as their caloric intake would imply. And as soon as they go back to their normal diet, the excess weight falls off.
What Bauer is saying is that obesity doesn’t arise from people suddenly eating more than their typical diet; it arises from some internal mechanism that drives the person to eat more.
Let me give you an example.
Take a typically lazy teenager. He sleeps till noon, lays around most of the day not doing much, and eats like a horse. Typically the wrong foods. Pizza, supersized soft drinks, and all sorts of crap. Yet he doesn’t get fat. Probably the most common comment I’ve heard from patients in my years of taking care of overweight people is about their kids. They say something along the lines of, “My kid is lucky. He/she can eat anything and everything and doesn’t gain weight. All I have to do is look at food, and I get fat.”
I would then always ask, “Couldn’t you do that, too, when you were his/her age?”
They always reflect a minute, then say, “Come to think of it, you’re right. I did do that.”
When kids are in their teens, their appetite (and lust for sleeping in) comes because they are going into and through puberty and remodeling their bodies. It’s all internally driven. They are hungry all the time (and sleepy), because they are growing. When they reach their adult body habitus, their appetite cools down and they don’t continue to gain weight.
At the time Julius Bauer was writing, obesity had pretty much been at a standstill in the low teens % in the US for decades. He and others attributed the small percentage of obesity to carb intolerance and a small handful of disorders that caused people to overeat, i.e., hypothyroidism.
One wonders what he would say about the obesity epidemic now? As I’ve discussed many times, there are a plethora of things that changed in the late 1970s/early 1980s when the obesity epidemic kicked off. People quit smoking, flour enrichment increased, seed oils and HFCS entered the scene in large amounts, carb intake went up, and countless other changes occurred. But these changes altered the interior workings of metabolism, which somehow drove people internally to eat more.
I kind of got carried away with this. My intent was to provide you with the 1941 Bauer paper and let you look at all the examples he provides of CICO not working. He wrote a slim book in the 1940s that I have a copy of stored away with my entire library. After being re-inspired, I need to go out and grab that from the storage unit. As I recall, it is full of useful information.
Here is a copy of his 1941 paper that I stuck in my dropbox. Also, (and I just remembered this) Mark Friedman et al wrote a paper last year that explained many, many situations in which CICO was falsified. You can pick any one of those to apply the Feynman quote and discredit CICO.
I would go over some examples, but I’ve about run out of room. I’ve gone on in Tolstoyian length, so let me cut it off. Maybe next week, we can go over metabolic fuel partitioning, which is the scientific term for what I’ve been talking about above.
Odds and Ends
Archaeologists discovered a silver amulet containing an 18-line text showing the oldest known devotion to Christianity north of the Alps.
The 10 most popular first names and their meaning. Michael (once a perennial top 10) dropped to 18th in 2024.
Why you should always 'take the money and run' if you win the lottery.
The treasurer hunter's (or maybe it's hoarder's) fear of doing exactly this probably explains why I have multiple boxes of junk in storage that need sorting before donating. What a find!
We put a very basic redwood sauna into our house in Boulder years ago that we didn't use nearly as often as we thought we would. But here's a high-end spa with a smorgasbord of sauna variations from a country that knows how to do the hot box right.
As a kid, Halloween was my favorite holiday, so these Vintage Halloween Postcards from the early 20th Century were like (black)catnip to me.
The era defining 25 food and drink trends of the first quarter of the 21st Century. Not sure what they say about us, but (dare I say it) food for thought.
A number of years ago the Bride and I applied for and got a pair of super discounted lifetime senior national park passes because we've always had a yen to tick off a visit to every park (figuring she, having been born and raised in one, gets us ahead of the game). But after reading these one-star reviews, we're not so sure. (Not really, but they're hilarious.)
Always keep an eye out when walking on the beach. If you're as lucky as this boy, that odd stone might just be a priceless artifact.
From the Dept of You've Got to be Kidding Me! Newest GenZ entrepreneurial dark horse is sperm racing. I am not making this up! See for yourself.
Only one of the 7 Wonders of the Ancient World still stands, with the other six destroyed by time, natural disaster, and disaffected youth. Leaving the ancients likely thinking: we just can’t have nice things! Some things never change.
And speaking of wonders of the ancient world. Though nobody really knows, here is a video of three competing theories about how the pyramids were built.
The rapper 50 Cent, adjusted for inflation. No surprise then that eggs, meat, and milk cost more, too!
Where did the stereotypical images of Halloween--hissing black cats and witches on broomsticks--come from? An interesting historical perspective.
Puns, shaggy dog stories, and corny Dad jokes are not modern inventions. Here’s a collection from the past, and they’ll be endless humorous to pre-teens, if you need a bit of levity or your storehouse of PG-rated groaners to entertain the grandkids/kids is running dry.

Video of the Week
Okay, this VOTW is a weird one. Not so much the video, but my reaction to it. Back in the early 1990s, I had never heard of an indie band called They Might Be Giants. I found out that, at that time, they were trying to write a song per day. I came across one of their albums titled Factory Showroom and purchased it. As it turned out, MD and I loved all of the songs on it. My particular favorite was Spiraling Shape.
I had a speaking gig in Dallas, so we drove down from Little Rock the afternoon before. We checked into our hotel and grabbed some dinner. At that time, there were no big box bookstores in Little Rock. And there is nothing more I like to do than roam a bookstore; and there is nothing MD hates more than doing the same.
So I dropped her back at the hotel and took off for either a Barnes & Noble or a Borders (Back when Borders existed). I roamed the store for an hour or so, and headed back to the hotel.
I slipped the They Might Be Giants CD in the player (tells you how long ago it was) and started driving back. I put Spiraling Shape on replay and cranked the volume. As I drove on the freeway, I became…I don’t know the word to describe it. It wasn’t exactly psychotic, but it was definitely a different brain wave than my normal one. Next thing I knew, I was flying down the freeways, going from one to another (and this was before I was familiar with Dallas and before there was a GPS system.) I had no clue where I was—I just kept driving in whatever altered state I was in caused by the music, the car lights, and who knows what? I finally settled down and made my way back to the hotel. But I’ve never had an experience like that since. And I certainly hadn’t had one before. Totally, totally weird. I listen to the song now, and it doesn’t do anything like that for me. But that one night…
Time for the poll, so you can grade my performance this week.
How did I do on this week's Arrow? |
That’s about it for this week. Keep in good cheer, and I’ll be back next Thursday.
Please help me out by clicking the Like button, assuming, of course, that you like it.
This newsletter is for informational and educational purposes only. It is not, nor is it intended to be, a substitute for professional medical advice, diagnosis, or treatment and should never be relied upon for specific medical advice.
Thanks for reading all the way to the end. Really, thanks. If you got something out of it, please consider becoming a paid subscriber if you aren’t yet. I would really appreciate it.
Finally, don’t forget to take a look at what our kind sponsors have to offer. Dry Farm Wines, HLTH Code, Precision Health Reports, and Jaquish Biomedical.
And don’t forget my newest affiliate sponsor Lumen. Highly recommended to determine whether you’re burning fat or burning carbs.
Reply