- The Arrow
- Posts
- The Arrow #273 Fraud, Ivermectin, and ApoB
The Arrow #273 Fraud, Ivermectin, and ApoB
Michael Eades
April 07, 2026
Greetings everyone.
I hope those of you who celebrate it had a lovely Easter weekend.
This issue of The Arrow is going to be a bit eclectic. A few of the topics have been inspired by my lovely bride, Mary Dan Eades. (Mary Dan is a name in the old Southern tradition of two first names, as in Mary Beth or Mary Rose. I started calling her MD early on in our relationship, and now almost everyone else who knows her does too.) The first is a commentary on a Ted Gioia Substack post about a miserable health issue he experienced. And got successfully treated. The thing I found surprising was how difficult it was for him to get his issue diagnosed.
I read the whole thing to MD. Before I got through the first brief paragraph, she had it diagnosed and said it aloud. It took me a little longer than it took her, but I did come up with the diagnosis in pretty short order. But MD is a helluva diagnostician, which is why all the children and grandchildren call her and not me when they need ‘the children’s pediatrician/doctor’.
She diagnosed a case of hookworm from a photo sent to her by our niece, who had been vacationing in Mexico. MD told her to go to the ER and tell them her aunt is a doctor and thinks she has hookworm. She did so, and the ER doc laughed at her. But when another (older) physician finally saw her, she ended up being diagnosed with hookworm. MD had never seen a case of hookworm in her life, but she remembered the telling features from her parasitology class in med school. (She has a steel-trap memory, whereas I have a mouse-trap memory. I’m always impressed (and insanely jealous) by her ability to recall.)
The second instance in which MD inspired me was through her monthly Zoom gig with MetFix, a successor to CrossFit. Every month she makes herself available to any and all MetFix trainers who have medical issues or who have clients with medical issues. I’m not directly involved, but she does her consulting on Zoom about six feet away from me, so I hear everything.
Over the last couple of months, almost all of the questions have been about ApoB and heart disease. I don’t know what has generated all this interest all of a sudden (actually, I do; and we’ll get to that later), but I figure if all these trainers are wondering about it, maybe readers of The Arrow are too. Consequently, I decided to do a deep dive on the subject to see if anything had changed since I last looked into ApoB (short version: it hasn’t) and present it below.
Before we get to all this, let’s look at a few other topics.
Blatant Academic Fraud
As most of you know, I don’t trust the medical literature a lot. I view most articles with more than a hint of suspicion and a handful of salt. I read them carefully, then check the references to make sure they really do back up the claims attributed to them. Even if everything checks out, I’m still a little leery unless I’m familiar with a given author’s work. I feel much better if multiple articles more or less support the one I’m reading.
Scientific fraud is rampant. It is common throughout the research hierarchy. It’s especially common in studies coming from China. A couple of days ago, I came across one of the most blatant examples I’ve ever seen. A guy whose videos I sometimes watch alerted me (and everyone else watching his video) to it. It is mind boggling in its temerity.
Here is the YouTube video.
Andy Stapleton is a PhD from the UK (I’m assuming, based on his accent and maybe I’m wrong), who creates videos on surviving the PhD process using various tools, especially AI. I’m guessing someone told him that to make interesting videos one has to over express and act bigger than life. If so, Andy took it to heart.
I find his videos interesting, but his over-the-top narration kind of drives me crazy. And, though his videos are 10-20 minutes long, he suffers a bit from the Curse of Knowledge. He assumes that everyone is as facile with using AI as he is. I often get lost in his explanations. So far, I haven’t used any of the tools he recommends, other than Perplexity. Which was how I found him. I searched for a tutorial on Perplexity and one of his videos popped up.
He posted a video a couple of days ago on this particular case of academic fraud that is almost unbelievable. I would never have found it, because I would never have been interested in the topic of the paper involved.
The paper, titled From Surgery to Strength: The Case for Mental Health Integration in Ileostomy Care, is not one I would have found on my own. It’s not a topic of interest to me. But I’m glad Andy Stapleton found it.
Don’t bother reading the paper – it was probably created by AI. The real giveaway is that the vast majority of references at the end don’t exist.
Let me show you what I mean. You can use this technique on other articles as well.
Scroll down the paper linked above until you get to the citations at the bottom.
The first one looks like this.
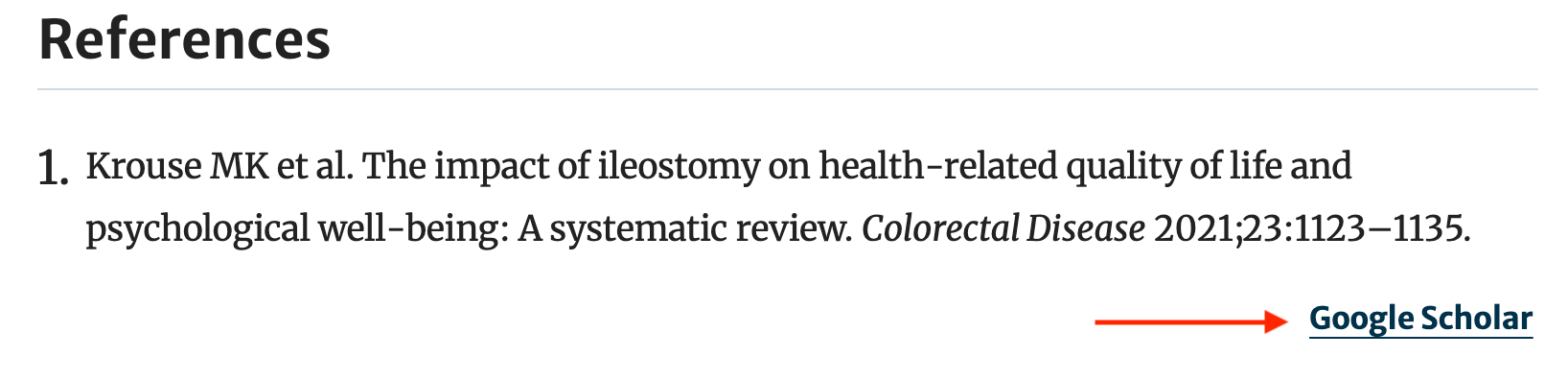
The red arrow added points to the Google Scholar link, which, when clicked, should take you directly to the paper in Google Scholar.
If you do click the link, here’s what you get.
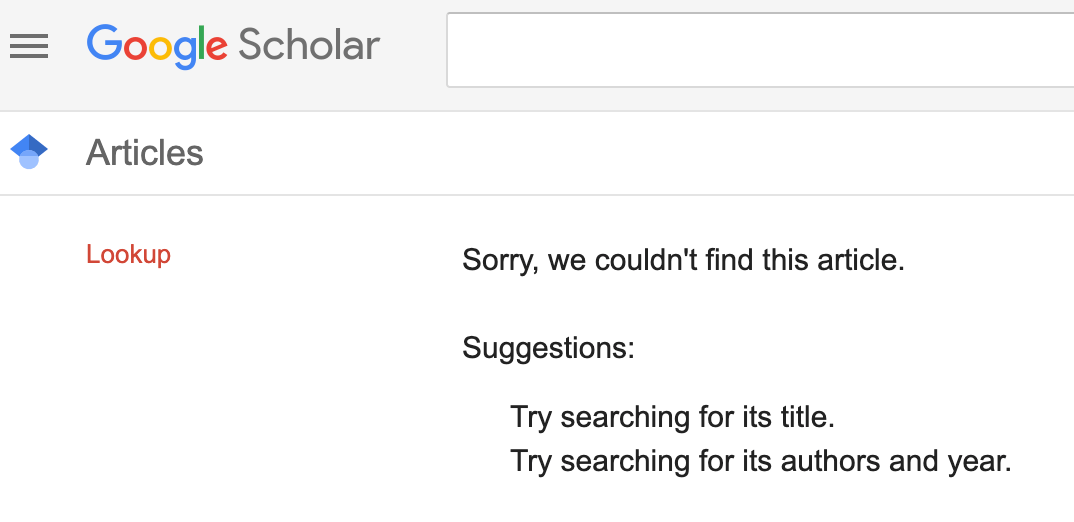
Then go through the lot of them and look at how many don’t exist. It’s a dead giveaway that the references, at least, were created by AI.
According to Andy Stapleton, the journal has been notified, yet the paper hasn’t been retracted. At least as of April 1, 2026, when I took the above screenshots.
This paper allegedly went through peer review and the journal’s editorial process.
The take-home lesson is to be aware of the potential for fraud and question everything you read.
Mercola Is at It Again
A reader emailed me a recent article Joe Mercola published titled High-Fat Diets Cause More Damage to Metabolic Health Than Carbohydrates (link). I think he’s gone off the deep end.
The reader who sent me the article sent it as a PDF. I wanted a link to it, so I went to Mercola’s site and searched for it. The search turned up all kinds of articles that were pro ketogenic dieting, pro fat, and generally favorable to the low-carbohydrate diet. But all of those articles were from a few years ago. Mercola has obviously had a nuutritional change of heart.
Here is the summary of the article in question.
-Mice fed high-fat and ketogenic diets developed rapid weight gain, rising blood sugar, and early liver damage within just two weeks, even when calorie intake matched higher-carbohydrate diets.
-High-fat feeding triggered fat buildup, inflammation, and scar tissue in the liver, while a high-carbohydrate diet didn’t produce the same level of liver injury.
-Excess dietary fat altered chemical “switches” on key metabolic enzymes, disrupting antioxidant systems and cellular energy production at the molecular level.
-Male mice showed greater insulin resistance and metabolic disruption than females on a high-fat diet, highlighting that biological sex influences how your body responds to excess fat.
-Reducing fat intake, eliminating seed oils and restoring balanced carbohydrate intake supports mitochondrial energy production and helps reverse the oxidative stress caused by fat-heavy diets.
The entire article is about a study on mice, not humans. Mice are not just furry little humans; they are way different from humans in countless respects. Mice are inexpensive, so are often used in studies before even rats, which are more expensive. Mice are right above invertebrates in the research food chain.
Since mice are so inexpensive, they are often used in preliminary studies to test a particular hypothesis. If the hypothesis holds in mice, then the next step up the ladder is to rats. Then, ultimately, to humans.
More often than not, what holds true in mice studies does not hold true in human studies. For one example we’ll discuss later in the ApoB section, resistin, a cytokine, is a completely different substance in rodents than in humans. All of the rodent studies on resistin, of which there are a number, do not apply to humans.
Reading the Mercola article reminds me of a sort of obscene, but funny, suggestion of a friend of mine years ago. My friend, his wife, MD, and I were having dinner at a Chinese restaurant. When the fortune cookies arrived at the end of the meal, the friend said if we added “in bed” to the end of whatever the fortune said, it would make it hilarious. Which it does. But now I can’t look at the little fortune slip from a fortune cookie without doing so. Try it in the fortune below.

Image by ClassicallyPrinted from Pixabay
We should all do a similar operation when we read mouse studies. At the end of everything posited, we should add “in mice.”
Go up and add “in mice” to the end of all the statements in the quote above. It makes the claim a lot less persuasive than it seems without that ending.
You should always look at human studies before believing claims from rodent studies.
I never tire of recommending the work of the Public Health Collaboration (PHC) in the UK, a non-profit that, among other things, tabulates all the human studies on weight loss and diabetes comparing the outcomes of low-carb diets vs low-fat diets. To be included, the studies must be carefully controlled, have a certain number of participants, and be of a defined length.
When compared, the low-carb diet absolutely crushes the low-fat diet in terms of outcomes.
So far, the PHC has found 71 studies that meet its criteria for inclusion. The results speak for themselves.

Here is the same data in infographic form.

If you would like to keep up with the PHC RCT data, use this link.
Almost always, weight loss on any diet corresponds with metabolic improvement, but even more so on low-carb diets as insulin levels are generally lower. The take-home message is to always look for human studies if you’re interested in human metabolism.
Ivermectin: The Wonder Drug
Remember back in the dreadful days of COVID how if anyone mentioned the drug ivermectin as a treatment, Fauci and others of his ilk came out of their burrows to condemn it mightily. (If you’ve forgotten how bad things were during COVID (and I had), read this.) The reason they condemned ivermectin and any other drug that might have treated COVID was to protect the Emergency Use Authorization (EUA), which allowed the mRNA COVID vaccines to be rolled out to the public without going through the standard FDA process.
If an infectious disease – or any other disease, one supposes – afflicts the population, an EUA allows a treatment for it to be brought to market without the full testing other drugs or treatments have to go through. The only proviso is that no other treatment is available for the given disorder. If one or more are available, then no EUA may be authorized.
Given the number of billionaires created by the mRNA COVID shots, it should come as no surprise that ivermectin, hydroxychloroquine (which was shown by Fauci’s own agency to be effective against SARS-CoV-1), and any treatment proposed for COVID would be ripe for quashing. If there had been no EUA, then COVID would have probably run its course long before the mRNA shots could have come to market.
Consequently, it was essential that any drug of any kind that could be shown to treat COVID be demonized. Ivermectin was an easy target because it was primarily known as an antiparasitic drug, so was easy to disparage as a horse dewormer or worse.
The mainstream media (or the trad media, a term I like better) were totally aboard the anti-ivermectin train. And, of course, the dimwitted audience yucked it up. Take a look.
The result of all this politicization spilled over into the scientific community. Instead of investigating the purported therapeutic claims for the drug (which did, after all, win a Nobel prize), they scrupulously avoided it to protect themselves against the negative politics.
In the video below, you can watch Tom Seyfried, one of the most I-don’t-give-a-shit-what-others-think scientists I know, refuse to touch it due to the politics involved.
(I’ve cued the video to the right spot, but the platform I use for The Arrow sometimes doesn’t pick up the cue. So if it starts at 0:00, go to 22:52)
My friend Professor Ben Bikman has recorded an excellent and thorough video on the discovery and many uses of ivermectin. I encourage you to watch it. You won’t be disappointed. I, myself, didn’t know a number of situations in which ivermectin could be a useful treatment.
And then there is this…
I really don’t know what to make of it. I’ve tried to find the data, but I can’t. I don’t think Bret would lie through his teeth about this, but I would really like to see the actual data. Watch it, but buyer beware.
The take-home message on ivermectin…
When the dust finally settles on the COVID era, ivermectin stands as a lesson in how science can be throttled by politics and perception. A drug once hailed as a “wonder” by Nobel laureates became a punchline—not because it failed, but because it threatened convenient narratives. The takeaway is simple yet sobering: truth in medicine doesn’t hinge on popularity or profit. It hinges on courage: the courage to look where others are afraid to and to ask questions long after the cameras stop rolling.
If you would like to support my work, take out a premium subscription (just $6 per month).
Trigeminal Neuralgia
One of my favorite newsletters on Substack is written by Ted Gioia, who writes about music, books, business, artificial intelligence, and the world in general. He recently veered from his normal subject matter into his own medical condition.
Here is his opening paragraph. (Actually, two, but the first is just one sentence long.)
I never talked about my pain.
For a start, it sometimes hurt too much to talk about anything. On bad days, any movement of my mouth—to speak, to eat, to brush my teeth—could trigger a jolt like an electric shock across the right side of my face. It felt like my cheek and lower jaw had been taken over by the vengeful Norse god Thor, who defended his turf with an endless supply of lightning bolts.
After I had read it myself, I was reading the post to MD. The bolded line above was as far as I had gotten when she exclaimed “trigeminal neuralgia!” It had taken me a bit longer to figure it out myself, but not all that long.
Ted Gioia at first thought it was a bad tooth, but an oral surgeon assured him his teeth were fine.
After multiple attacks of severe pain, he decided to do the research himself to figure out what was going on.
I now knew that I needed to take action. But what kind of action? I still didn’t know what was wrong with me. But I did possess one skill that could help—I’m very good at doing research. So I set myself the task of diagnosing myself.
A few months later, when I laid it all out for my neurologist, she was amazed. “Are you a professional medical researcher?” She asked.
“No,” I replied. “But I am a writer, and I have spent most of my life doing research of various sorts.”
“Well, what you did was impressive.”
If he had gone to just about any doctor before doing all his research, I suspect he would have gotten a diagnosis pretty quickly.
Every doctor who has gone through medical school learns about the cranial nerves, one of which is the trigeminal nerve.
The cranial nerves originate in the base of the brain and are famous for the mnemonic medical students use to memorize them. On Old Olympus’s Towering Top, A Finn And German Viewed Some Hops. The cranial nerves are also defined by number. The mnemonic above lists them in numerical order as well. The bolded first letter of each word above corresponds to both the first letter of each cranial nerve in numerical order. Below is a graphic from the Cleveland Clinic showing both name and number, but a couple of them have different names than they did when I learned them.

As you can see, the mnemonic doesn’t work for cranial nerves VIII and XI. Number 8 used to be called the Auditory nerve, and number 11 was formerly called the spinal accessory nerve. They’ve dropped the “spinal” part of the last one. Number 8 has been changed completely.
I’m sure there is a new mnemonic for the current names, but I don’t know it. I can still remember all the cranial nerves as I learned them decades ago by the mnemonic. I’m pretty sure docs who learned them later can remember them as well.
The trigeminal nerve exits in front of the ear and breaks into three separate portions that spread throughout the face.
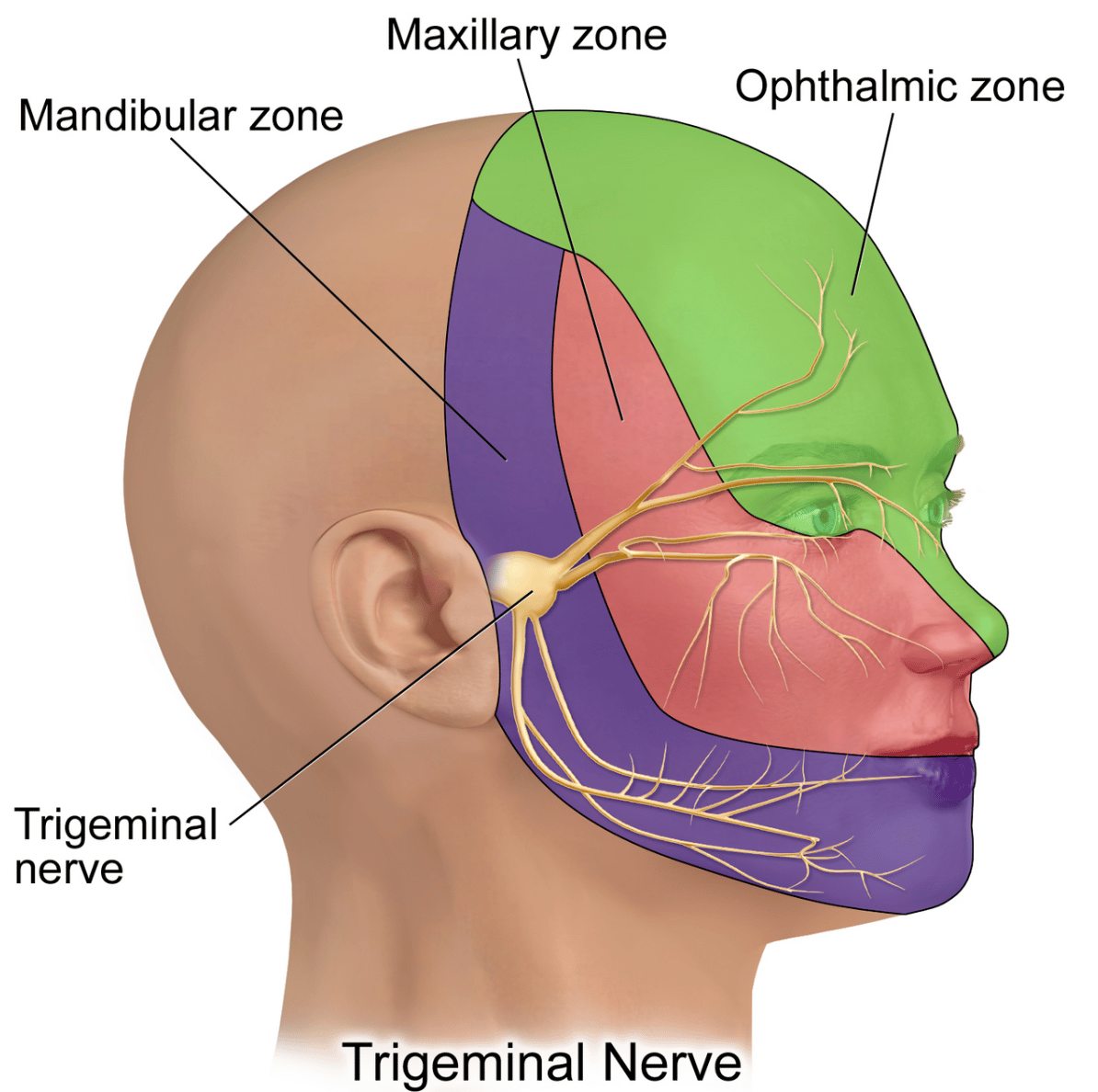
As you can see from the graphic above, the lower branch of the trigeminal nerve serves the very spot from which Ted Gioia’s severe pain emanated.
Although Ted spent a lot of unnecessary time trying to diagnose himself, he did exactly what I would have done in his place once I had the diagnosis. He used his research skills to find the best specialist to treat his problem.
My intention with this section of The Arrow is not to do a deep dive on trigeminal neuralgia. The disorder is not all that common, but it is more common than Ted made it out to be. And it can be a serious and debilitating condition. The good news is that with the right diagnosis and the right practitioner, there is real help available. I’ve posted this section as a public service notice, so anyone who might have the same symptoms as Ted or an actual diagnosis of trigeminal neuralgia can know how to find the right practitioner to diagnose and treat it. (Just go to the link at the start of this section to read his Substack about it, and relief could be a click away.)
The ApoB Team
For over a century, researchers have been measuring blood cholesterol, but it wasn’t until the 1950s and 1960s that the measurement came into more common use. Driven, I’m sure, by the Ancel Keys’ theory implicating blood fats as drivers of heart disease. By the 1970s, lipoproteins, the carriers of cholesterol (more about which later) were fractionated into various particle densities based on weight.
Triglycerides – fats in the blood – were measurable in the 1950s-1960s, but also didn’t come into common use until later.
Both cholesterol and triglycerides are lipids, i.e., fats. Triglycerides are fats in the way we all think of fats; they are primarily used as energy for the cells. Cholesterol is a waxy kind of fat used by the body as a precursor for a number of important hormones — sex hormones and adrenal hormones, to name a couple. Importantly, cholesterol is also a structural fat. The body uses it to help maintain the necessary rigidity of the cell membranes.
If it weren’t for structural support of cholesterol our cell membranes would collapse. To put it in Shakespearean terms, if there were no cholesterol, our bodies would quickly “resolve [themselves] into a dew.” Cholesterol is so important to life that virtually all cells can produce it if needed, although most is made in the liver.
Since both triglycerides and cholesterol are fats, neither mixes well with water, which is the main component of blood. And that creates a bit of a dilemma.
Most of us have had the experience of plunging a hot skillet used to cook, say, bacon into a sink of steaming water. Some of the fat comes off the skillet and floats to the surface as fatty globs. If we add dishwashing liquid to the water, the fat breaks down and becomes soluble in the water. The dish soap creates a coating around the fat molecules that allows them to mix with the water.
In order to move freely through the blood to reach their needed destinations, both cholesterol and triglycerides need to be soluble in blood so they don’t float up in giant blobs like the bacon grease mentioned above. Nature has wrapped both the cholesterol and triglycerides in a carrier protein, a sort of coating that makes them soluble.
These protein-wrapped particles are named, logically enough, lipoproteins. You can think of lipoproteins as little boats transporting cholesterol and triglycerides to and from various tissues and organs.
Below is a simplified graphic of a lipoprotein:
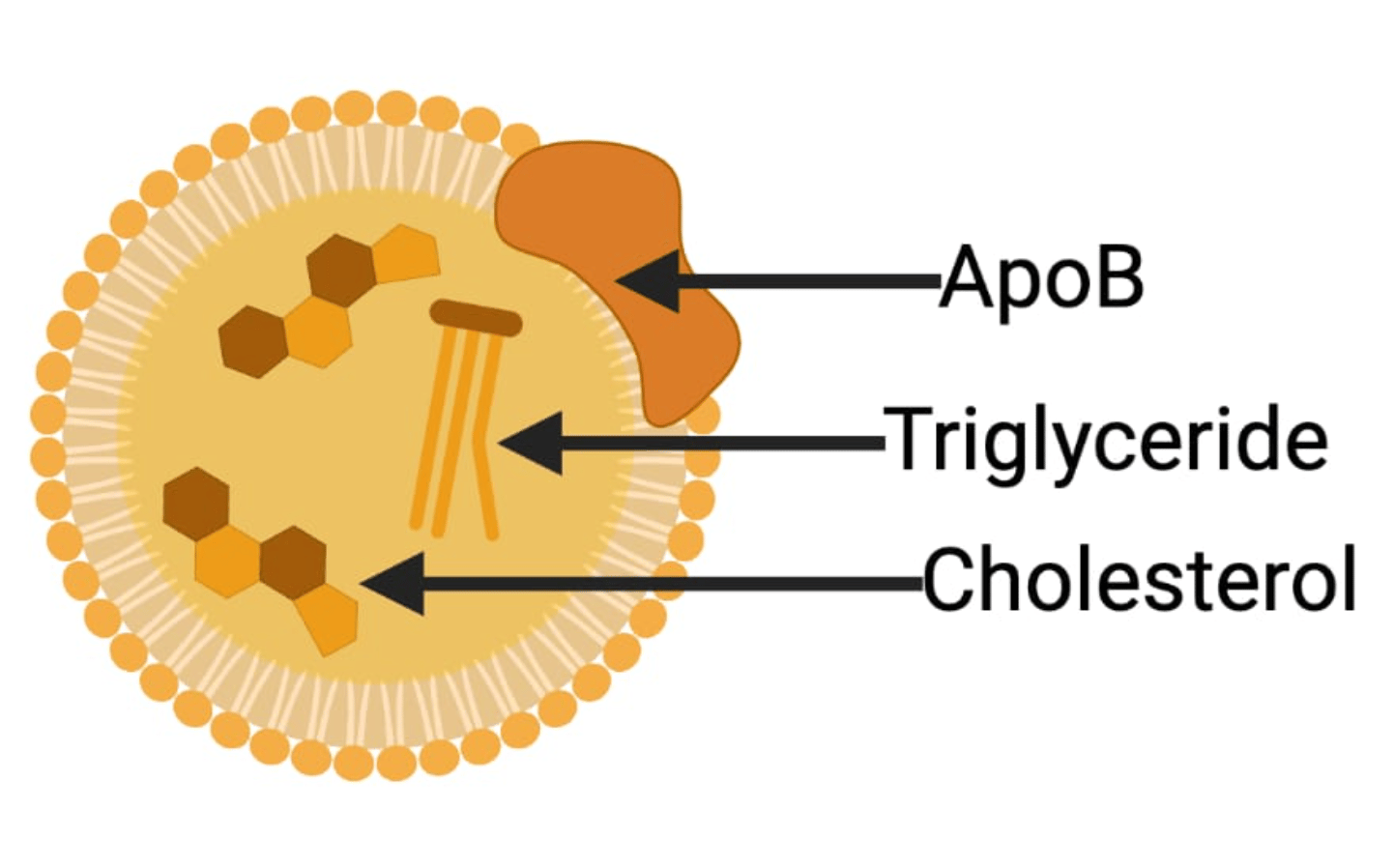
There are a number of these lipoproteins, all measured by density. LDL-C, stands for low-density lipoprotein cholesterol. Though LDL-C contains triglycerides along with the cholesterol, the particle itself is named for the cholesterol it contains. The same goes for VLDL-C, which is a very low density lipoprotein. And IDL-C (intermediate density lipoprotein) as well as HDL-C, (high-density lipoprotein).
To make it even more confusing, LDL-C, which is the most common way LDL-cholesterol is noted, represents the cholesterol contained in the lipoprotein particle. If it is the LDL particle under discussion, that is called LDL-P. I’ll use LDL-C when I’m talking about the cholesterol content of an LDL particle. I’ll use LDL-P, when I’m writing about LDL particles.
When the lab measures LDL-C, what it is determining is the actual cholesterol contained in all the LDL particles. LDL-C is difficult to measure, it is usually calculated using the Friedewald equation. It can be measured directly, but it is costly, so almost all LDL-C values are determined indirectly.
The lab measurement of total cholesterol is the measurement of all the cholesterol circulating in all the different lipoproteins.
Blood triglycerides are a measurement of all the triglycerides in all the circulating lipoproteins.
Because, doubtless due to the Ancel Keys' influence whereby lipids were entrenched in the minds of lipidologists and cardiologists as the driving force for the development of coronary artery disease, the search was on for a slicing and dicing of lipoproteins in every way possible to prove their role. The goal was to find some lipoprotein measure that would more strongly correlate with heart disease than cholesterol or even LDL-C.
Researchers figured out how to determine LDL particle numbers in the 1990s and those measurements came into use. As it turned out, LDL particle numbers correlated well with small, dense LDL particles. Which makes sense. And both predicted heart disease risk better than any of the other previous markers.
I well remember a conference MD and I attended at UT Southwestern in Dallas. All of the research luminaries from all over the world gave talks, primarily about diet and heart disease. The summary at the end of the talks was presented by Walter Willett (now retired) from Harvard.
He said (this is not a direct quote, but it’s close), Well folks, the data is in. The low-fat diet has been a failure. Much as all of us wanted it to work, it hasn’t been shown to be at all successful in the prevention of heart disease. In fact, it’s been the opposite. We can lower cholesterol levels by putting patients on high-carb, low–fat diets, but they end up worse overall because their LDL-cholesterol converts from the big fluffy kind to the small, dense kind, which is a much greater risk factor.
At the time, as we sat in the audience, MD and I both figured Willett’s summary might effectively kick off the low-carb era.
But we were wrong.
Why?
As I’ve said many times, the pharmaceutical industry drives the medical industry.
Shortly after this talk, statins hit the scene, and there was no looking back. Since statins lowered LDL-C, LDL-C became all the rage. That was the blood marker that counted. Particle size and particle number fell by the wayside.
Everyone began to focus on LDL-C simply because there was now a drug to reduce its levels.
In most of our own patients on low-carb diets, we found LDL-C levels declined (had they been elevated in the first place) by the time of their first lab recheck in six weeks. But occasionally we had patients whose LDL-C levels increased. In those cases, we told them that the odds were that their LDL particles had gone from the small, dense variety to the larger, fluffy kind. We offered to get their LDL particle size measured to make sure, but told them it was an expensive test and that their insurance might not cover.
Most took our assurances, but a few wanted to get the test. In every case, we found an increase in LDL particle size. In other words, they had shifted from smaller, denser LDL particles to the big, fluffy ones.
Just a side note before we go on with this session. Most people don’t realize that LDL is a part of the innate immune system, something I’ll explore in a later post. There is much evidence from multiple studies that lipoproteins may prevent bacterial, viral, and parasitic infections. They can also detoxify lipopolysaccharide and lipoteichoic acid, both endotoxins that bacteria can release causing many emergency health issues and even death. Most of this work is done by the large, fluffy LDL particles. Just another reason to follow a low-carb diet.
Okay, now finally to ApoB…
ApoB is a protein attached to all lipoproteins. There is one and only one ApoB on the surface of each lipoprotein particle. By counting ApoBs, labs can now determine with accuracy the total number of lipoprotein particles of every stripe in circulation.
The ability to measure ApoB came into common use in the 1990s. But with the tsunami of statins not long after, most people forgot about ApoB. Statins drove down LDL-C much more than they did ApoB, so LDL-C became the major marker everyone began to focus on.
But then, as inevitably happens with all pharmaceuticals, the statin patents expired. The drugs then could be produced as generics. And the prices for statins plummeted.
As mentioned above, Big Pharma more or less directs the way medicine is practiced.
The drugs known as PCSK9 inhibitors came on the market and lo and behold these drugs reduced ApoB levels significantly more than statins did, so now ApoB is all the rage. Statin prescriptions now cost less than $300 per year in the US, while a year’s worth of PCSK9 inhibitors run around $5,000 per year.
Despite the fact that testing for it has been around for decades, suddenly everyone is obsessed with ApoB, and it’s no wonder. Treating it once again puts big bucks in the pockets of Big Pharma. Big bucks they lost when statins went off patent. All by worrying people over a lab value. Treating a number, not a disease. I’ll discuss the real disease in a bit.
I’m posting the video below for those who want to get into the real nitty gritty of the lipid world. The video shows the entirety of lipid metabolism from the gut to the sex hormones. It is comprehensive and fascinating, at least for folks who like this sort of thing. But I warn you; it is long. A little over an hour. If you want to see the part about ApoB, it starts around the middle of the video.
For those who may have an interest in what goes on in medical school, this video is typical for a single lecture. The guy giving the whiteboard lecture in the video does a much better job than most med school profs. What you need to remember re med school is that every pathway he presents and every enzyme he lists catalyzing each reaction (there are many) are all fair game for test purposes. Also, there are three or four lectures like this one every day, five days per week for the entire first two years of medical school. It is not a cake walk.
Having been to engineering school before I went to med school, I studied for my first med school test by learning concepts, as we did in engineering. And I ended up getting the lowest grade in the class on that test. I quickly realized I had to change my way of studying. Instead of learning concepts, I started memorizing pathways and names and minutia. That’s what it took to get through.
One of the interesting parts of this video is when the guy presenting it refers to LDL-cholesterol as ‘the bad one’. He does so after describing all the pathways by which LDL works, all of which have a purpose. Then, without any explanation, he tells us that LDL is the bad one. But he doesn’t tell us why. I suspect he’s simply parroting what he’s heard. Don’t let that put you off the video, though. It really is excellent if you want to know the ins and outs of lipid metabolism.
Back in 1997 when I was just coming to the realization that the lipid hypothesis of heart disease was incorrect, a paper came out in Circulation, a top notch cardiology journal, titled Fasting Triglycerides, High-Density Lipoprotein, and Risk of Myocardial Infarction (My Dropbox link) that helped sharpen my thinking.
The paper evaluated the different lipid measurements and found the one most predictive of the development of heart disease was the triglyceride to HDL ratio (TG/HDL). Other researchers found the same thing and published their results. Then a few years later a large prospective/meta‑analytic paper then confirmed and quantified the association across hundreds of thousands of people followed over time.(Link)
What I knew from my own clinical experience with many, many patients following low-carb diets was that those diets brought about a marked reduction in triglycerides and an elevation in HDL, the combination of which reduced the TG/HDL ratio. Which followed the medical literature. There were many papers showing the restriction of carbohydrates brought about a rapid reduction in triglyceride levels. Not as many papers showed an increase in HDL with an increase in dietary fat intake, especially saturated fat, but some did. I didn’t find any that showed an increased consumption of fat lowered HDL levels.
Since this fairly rapid change in the TG/HDL ratio occurred before a lot of weight was lost, I reasoned that it wasn’t the decrease in triglycerides or the increase in HDL that decreased the likelihood of developing heart disease, but instead that the changes in those markers represented an overall improvement in metabolic function.
As it turns out, improved metabolic function reduces ApoB just like it does with an increased TG/HDL ratio.
ApoB as a Marker of Metabolic Dysfunction
Think of ApoB as a readout of how well your liver is managing the daily flood of fat and sugar coming in from your bloodstream. Under normal, insulin-sensitive conditions, the liver efficiently packages and exports only as many lipoprotein particles as the body needs. But when insulin resistance develops — whether from excess visceral adipose tissue, chronic high carbohydrate intake, or both — the liver loses its sensitivity to insulin's normal "slow down" signal. In a healthy state, insulin triggers the degradation of newly formed ApoB before it can be assembled into a VLDL particle; in an insulin-resistant liver, that degradation pathway is blunted, so more ApoB survives and gets packaged into circulating particles. The result is a higher output of VLDL particles, which cascade downstream into elevated triglycerides, lower HDL, a shift toward small dense LDL, and, critically, a higher total ApoB particle count — the classic atherogenic dyslipidemia of metabolic syndrome.
As I mentioned in the section above re Dr. Mercola, resistin is a protein involved in the creation of ApoB. In rodents, resistin is secreted almost entirely from fat cells, so it rises in direct proportion to fat mass (I’ll add, “in mice”). In humans, resistin is secreted mainly from macrophages, not directly from fat cells, but from the macrophages accumulated in the visceral adipose tissue. Because visceral adipose tissue accumulation is an inflammatory process, it draws macrophages to put out the fire.
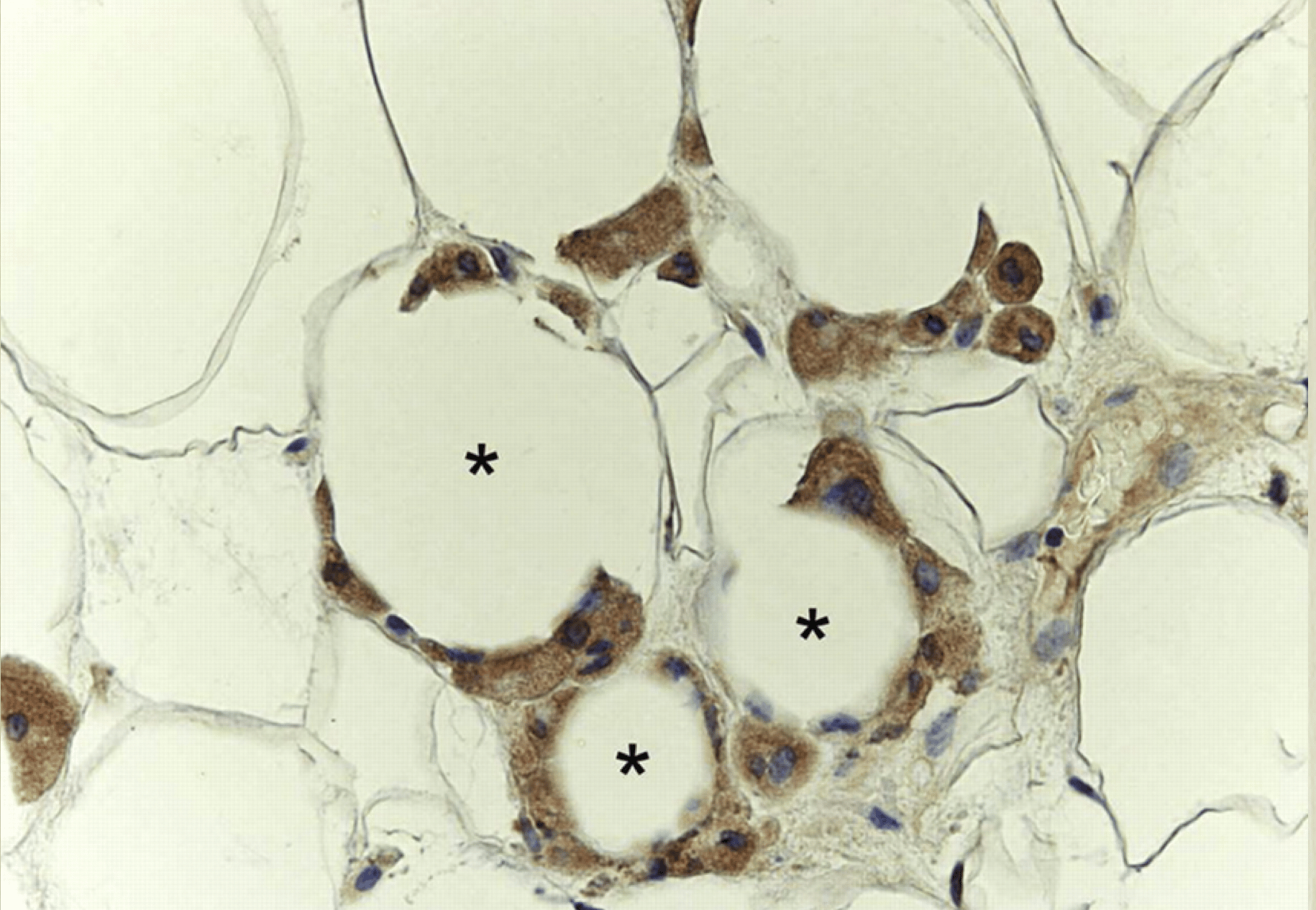
These macrophages accumulated in the visceral adipose tissue release resistin, a protein that activates a complex process that ends up increasing ApoB. As we discussed in an earlier newsletter, macrophages can make up half the mass of adipose tissue, which can produce a lot of resistin. See the graphic below showing macrophages in dark invading the adipose cells.
How a Low-Carbohydrate or Ketogenic Diet Acts on This System
Reducing dietary carbs attacks the increased ApoB problem at several points simultaneously.
First, lower carbohydrate intake reduces insulin secretion, which directly lowers the chronic hyperinsulinemia that drives hepatic insulin resistance, allowing the liver's normal ApoB degradation pathway to partially recover.
Second, carbohydrate restriction sharply curtails hepatic de novo lipogenesis , the process by which excess dietary carbohydrate — especially dietary fructose — is converted to fat in the liver that then fuels VLDL assembly, the process whereby the ApoB is attached to the developing lipoprotein.
Third, as fat mass is lost (particularly visceral and hepatic fat), the inflammation that elevates resistin resolves, shifting the liver's biochemical environment toward lower VLDL output.
The clinical result, well-documented in patients with insulin-resistant dyslipidemia, is a reduction in triglycerides (often the most dramatic and reliable lipid change), a rise in HDL, a shift toward larger, less atherogenic LDL particles, and a reduction in ApoB. A paper from 2022 shows this process nicely. A randomized controlled feeding trial specifically demonstrated that a low-carbohydrate diet high in saturated fat improved insulin-resistant dyslipoproteinemia and lowered Lp(a), without adversely affecting LDL-C.
Having written the above, I’ve got to tell you that it doesn’t apply to a small contingent of people called lean-mass hyper-responders. I’ve discussed these folks before, and I’ll discuss them again down the road once the dust settles from the latest paper, which is now mired in controversy.
But most of us are not lean-mass hyper-responders, so the metabolic pathways discussed above do apply.
The takeaway message…
The population where the discussion above matters most are people with metabolic syndrome, visceral adiposity, insulin resistance, and atherogenic dyslipidemia. In that context, a well-formulated low-carbohydrate or ketogenic diet addresses the upstream metabolic drivers of elevated ApoB rather than simply masking the number with a drug.
A lot of prime steaks can be had for the $5,000 per year spent on PCSK9 inhibitors. Which reminds me, I didn’t get around to the description of how these expensive drugs work because this edition has already gone on to Tolstoyian length. I’ll discuss and explain in an upcoming issue.
Odds and Ends
A worthy use for soybeans. Well, this and BioWillie.
I've ridden (and cleared) plenty of trails back in my college summer job as a US Forest Service Ranger. And I love the outdoors. But I've never been much of a hiker for the sake of just taking a hike. If there's something worthwhile to see at the end of the trail, then OK; I’ll boot up. I get it. And some of these Best Hikes in the US are intriguing enough to make me willing to do it.
I feel fortunate to speak English as my native tongue, because with all its oddities and exceptions, it would be a 'beech' to learn to sort them out and pronounce them all properly coming at it as a second language. And here's why there's so much confusion.
The Thomas Moran painting that inspired a national park. I could look at his works for hours. I probably have.
Apparently it takes a village to birth a sperm whale calf. First ever footage of its kind. Who knew it was such a family affair?
Kids may not be taught cursive writing anymore (a great tragedy IMHO and MD’s) but perhaps they could lean into some creative cursery. I've heard some of these colorful vintage curse words to be sure, but not all.
The press for NBS goes on... Hershey's to produce actual chocolate again!
Favorite Easter Candy by state. If I were going to indulge, I'd pick Cadbury's Eggs, although it doesn't jibe with the preferred candy of the state of my birth (MO) or any state I've ever lived in. The Bride would pick Whoppers (the AR fave and the state of her birth) or M&Ms (the favorite of a neighboring state to AR). I confess I don't even know what a couple of them are! What's yours?
The Happiest City in the World? Maybe. MD and I have only been there once, and it was perfectly enjoyable. We had a fantastic meal with some business colleagues. But the criteria of what constitutes 'happiness' in this survey is curious. But then happiness is a tough attribute to measure. https://www.afar.com/magazine/the-happiest-cities-in-the-world

Video of the Week
When this popped up on my YouTube feed, I knew I had to post it. No commentary needed. What a classic. Just enjoy!
Time for the poll, so you can grade my performance this week.
How did I do on this week's Arrow? |
That’s about it for this week. Keep in good cheer, and I’ll be back soon.
Please help me out by clicking the Like button, assuming, of course, that you like it.
This newsletter is for informational and educational purposes only. It is not, nor is it intended to be, a substitute for professional medical advice, diagnosis, or treatment and should never be relied upon for specific medical advice.
Thanks for reading all the way to the end. Really, thanks. If you got something out of it, please consider becoming a paid subscriber if you aren’t yet. I would really appreciate it.
Finally, don’t forget to take a look at what our kind sponsors have to offer. HLTH Code, Precision Health Reports, and Jaquish Biomedical.
And don’t forget my newest affiliate sponsor Lumen. Highly recommended to determine whether you’re burning fat or burning carbs.
Reply